

1. Understanding the concept of a mechanical lock
The course of the pudendal nerve requires passage through anatomically narrow regions. Under physiological conditions, these zones do not cause pain. They become mechanical locks when their geometry is unfavorably altered (posture, repeated constraints) or when surrounding tissues lose their adaptive capacity (Robert et al., 1998).
A mechanical lock is not necessarily a lesion. It may correspond to an area where the nerve is challenged by intermittent compression, friction, or repeated shear. This explains a frequently fluctuating clinical picture: exacerbations during sitting, relief with unloading, and variability according to activities and duration of exposure to constraints (Labat et al., 2008/2023).
In pudendal neuralgia, symptoms do not always indicate a “lesion,” but may reflect an unfavorable mechanical context in which the nerve is stressed beyond its adaptive capacity (Labat et al., 2008/2023).
2. Ligamentous pinch: the pivotal conflict
The pudendal nerve crosses a critical region near the ischial spine, in close proximity to the sacrospinous and sacrotuberous ligaments. This region constitutes the ligamentous pinch, described as a major anatomical mechanism of nerve irritation (Robert et al., 1998).
A distinctive feature of this conflict is its strong posture dependence. During prolonged sitting—particularly with pelvic retroversion (“posterior pelvic tilt”)—ligament tension may increase, reducing the space available for the nerve and amplifying compression and shear forces (Labat et al., 2008/2023).
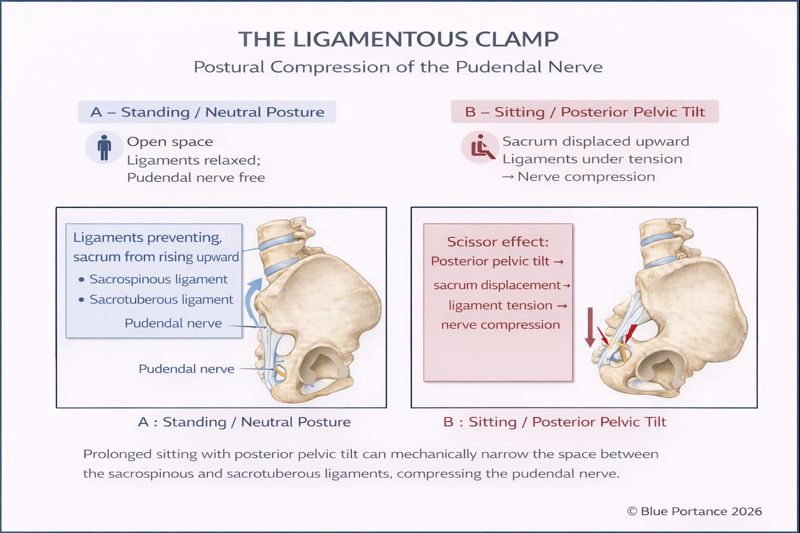
This model explains a classic feature: symptom aggravation while sitting. It does not imply that sitting is the “sole cause,” but that it may act as a constraint factor revealing or maintaining a pre-existing conflict (Labat et al., 2008/2023).
3. Alcock’s canal: a constrained anatomical tunnel
After the ischial spine region, the pudendal nerve travels within Alcock’s canal, a fascial tunnel formed by a duplication of the fascia of the obturator internus muscle (Robert et al., 1998).
In this Knowledge Base, Alcock’s canal is approached as a mechanical lock: a limited space where the nerve and accompanying vessels may be exposed to increased mechanical stress when tunnel volume is reduced or when surrounding tissues become hypertonic (Cholewa et al., 2024).
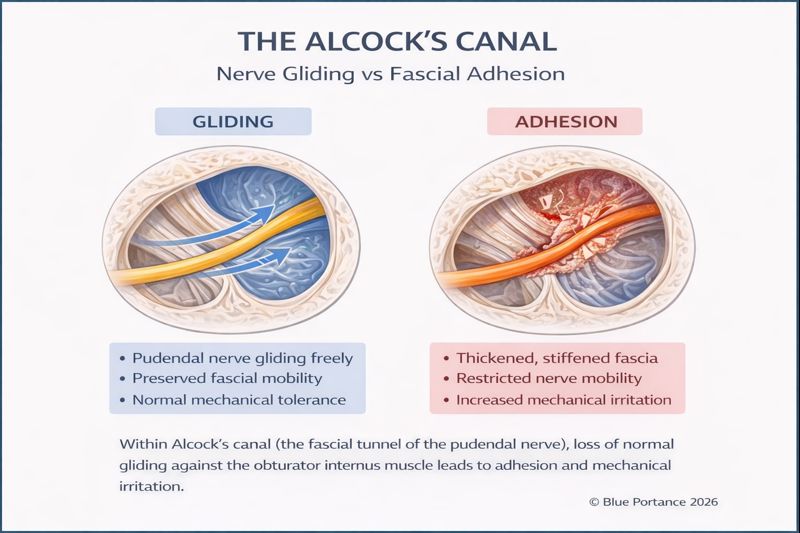
An essential BDC reading point: nerve involvement within Alcock’s canal may result from a strictly “geometric” mechanism (lock), or from a subtler mechanism of reduced tissue mobility. This distinction is addressed in the triage and fascia pages (Stecco & Stecco, 2024).
4. Cumulative locks and symptom variability
Mechanical locks rarely act in isolation. A moderate conflict at the ligamentous pinch may become symptomatic when combined with a constraint within Alcock’s canal, or when associated with protective muscular hypertonia (Cholewa et al., 2024).
This cumulative effect explains clinical variability: fluctuating pain, alternating calm periods and exacerbations, particular sensitivity to prolonged sitting, and differing responses depending on posture and context (Labat et al., 2008/2023).
Scientific references
- Robert, R., Prat-Pradal, D., Labat, J.-J., et al. (1998). Anatomical basis of pudendal nerve entrapment. Surgical and Radiologic Anatomy.
- Labat, J.-J., Riant, T., Robert, R., et al. (2008; updated 2023). Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria).
- Cholewa, J., et al. (2024). Myofascial entrapment in Alcock’s canal: the role of pelvic floor hypertonia.
- Stecco, A., & Stecco, C. (2024). Fascial densification and neuropathic pain: clinical implications.