

1. Why triage is decisive
A large proportion of individuals suffering from pudendal neuralgia present with normal morphological imaging. The absence of visible lesions frequently leads to questioning the symptom itself, even though pain is intense and disabling (Labat et al., 2008/2023).
The SBNFA™ triage aims to avoid this dead end by establishing a clear distinction: neuropathic pain may result either from an objectively identifiable structural injury or from a functional dysfunction related to mechanics, tissues, and the nervous system, without anatomical rupture.
2. Structural injury: when a lesion is identifiable
A structural injury corresponds to situations in which an anatomical abnormality can be identified: post-traumatic injury, surgical sequelae, compressive mass, localized scar fibrosis, or bone abnormalities. These situations remain a minority in pudendal neuralgia, but they do exist (Robert et al., 1998).
In such cases, neuropathic pain is directly correlated with a stable anatomical modification. Imaging, specialized clinical examination, or targeted tests may provide convergent evidence.
Structural injury is not the rule in pudendal neuralgia. Its presence must be investigated, but its absence does not invalidate the reality of the symptom (Labat et al., 2008/2023).
3. Functional dysfunction: when pain exists without a lesion
The majority of pudendal neuralgia presentations fall under functional dysfunction. The nerve is neither severed nor compressed by a mass, but subjected to repeated mechanical constraints: prolonged posture, muscular hypertonia, fascial densification, and loss of tissue gliding (Stecco & Stecco, 2024).
These mechanisms are not visible on standard imaging. They manifest as mechanical hypersensitivity of the nerve, fluctuating pain, posture- and context-dependent symptoms, and progressive aggravation linked to nervous system adaptation.
Recent research on fascia and neuropathic pain shows that fascial densification and reduced tissue mobility may be sufficient to generate persistent nerve irritation, without visible anatomical lesions (Stecco & Stecco, 2024; Cholewa et al., 2024).
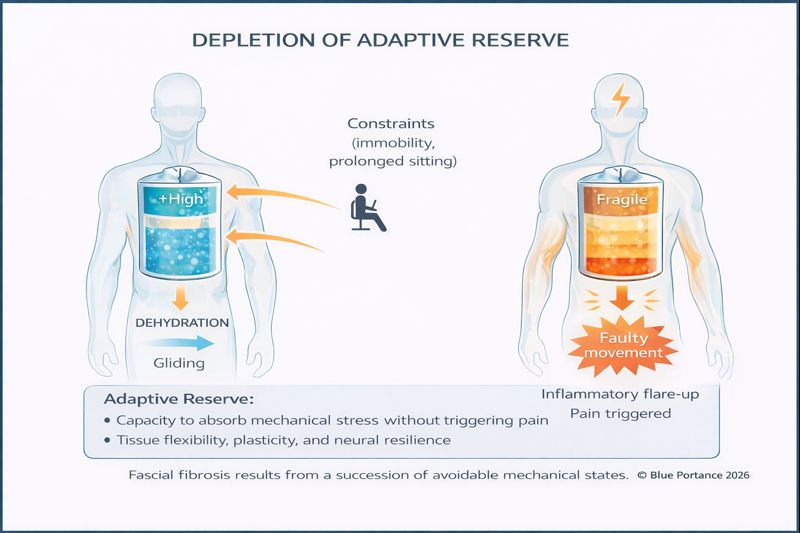
4. Adaptive reserve: how far the system can still compensate
In a functional dysfunction context, the presence of symptoms does not necessarily indicate a locked system. The pudendal nerve, surrounding tissues, and the nervous system initially possess an adaptive reserve: the ability to tolerate mechanical, biological, and postural constraints without transitioning to persistent pain.
This reserve relies on dynamic parameters: quality of tissue gliding, postural variability, absence of fixed constraints, neuromuscular modulation, and the capacity of tissues to rehydrate between mechanical loads (Stecco & Stecco, 2024).
As long as this reserve is preserved, the functional mechanisms described above may remain partially reversible. Symptoms are often fluctuating, posture-dependent, variable over time, and sensitive to contextual changes (duration of sitting, stress, fatigue, recovery).
Functional does not mean chronic. It becomes durably pathological when the adaptive reserve is progressively exhausted.
Repeated exposure to non-varied constraints — particularly prolonged sitting — progressively reduces this tolerance margin. Tissues lose their gliding capacity, protective hypertonia sets in, and micro-mechanical stress becomes sufficient to trigger increasingly early pain signals.
Exceeding the adaptive reserve thus constitutes a critical threshold: beyond this point, functional mechanisms no longer generate only contextual pain, but fuel a chronicization process involving central sensitization and tissue stiffening (Blue Portance — SBNFA™ Model, 2026).
© Blue Portance — 2026
5. SBNFA™ triage indicators
SBNFA™ triage relies on a constellation of indicators rather than a single criterion. Certain elements point toward a functional rather than a structural logic.
- Normal imaging despite intense and persistent pain.
- Marked postural variability (worsening while sitting, partial relief with unloading).
- Fluctuating pain depending on context, duration of exposure, stress, or fatigue.
- Mixed clinical presentations combining perineal, urinary, rectal, or genital pain without local lesions.
- Progressive onset without clearly identified initial trauma.
Conversely, strictly localized and stable pain, appearing abruptly after a precise event, more strongly suggests a structural injury requiring targeted investigation (Robert et al., 1998).
6. Structural, functional, and adaptive threshold: key distinctions
This table provides a comparative reading intended to clarify what falls under objectifiable structural injury versus functional dysfunction (without visible lesions), and why the concept of adaptive reserve often conditions the transition toward chronicity.
On mobile: scroll horizontally to view the table.
| Criterion | 🏗️Structural involvement | 🌊Functional dysfunction |
|---|---|---|
| Definition | An identifiable anatomical abnormality that can explain a local conflict. | Pain without an objectifiable lesion, related to an unfavorable mechanical regime (interfaces, gliding, protective hypertonia). |
| Common triggers | Trauma, surgery, scar tissue, mass, or a localized conflict. | Prolonged sitting, repeated constraints, protective hypertonia, densification of tissue interfaces. |
| Relationship to imaging | More frequent correlation between the observed abnormality and the symptomatic area. | Frequent decoupling: imaging may be normal despite severe symptoms (to be interpreted within a mechanistic framework). |
| Symptom profile | Tends toward more stable pain, sometimes less dependent on immediate context. | Pain is often fluctuating, strongly posture- and duration-dependent, sensitive to load variations. |
| Dominant mechanism | Local anatomical conflict (compression/irritation) associated with an identifiable structure. | Loss of mechanical compatibility between the nerve and its environment: reduced gliding, shear forces, repeated micro-aggressions. |
| Typical orientation logic | Approaches targeting an objectified anatomical abnormality (e.g., localized procedure, specialized exploration). | Approaches aiming to modulate mechanical and tissue constraints (posture, mobility, gliding, reduction of protective tension). |
| Clinical example | Pudendal conflict associated with post-surgical scarring or localized fibrosis. | Posture-dependent presentation (prolonged sitting, cycling) with hypertonia and loss of gliding without visible lesion. |
| Adaptive reserve | Often limited by the anatomical constraint: the compensation margin may be reduced from the outset. | Variable and decisive: as long as it is preserved, the system remains modifiable; its exhaustion marks a threshold toward chronicization. |
| References | Robert et al. (1998) | Stecco & Stecco (2024) ; Cholewa et al. (2024) |
7. Clinical implications and understanding chronicization
The absence of clear triage promotes diagnostic wandering: repeated negative tests, inappropriate treatments, misunderstanding, and loss of confidence. This wandering contributes to chronicization through protective hypertonia, central sensitization, and progressive tissue stiffening (SBNFA™ Model, Part IV, 2026).
The SBNFA™ triage does not aim to exclude a structural origin, but to recognize the central role of functional mechanisms in the majority of pudendal neuralgia cases, and to restore explanatory coherence when lesions are not visible.
Scientific references
- Labat, J.-J., Riant, T., Robert, R., et al. (2008; updated 2023). Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria).
- Robert, R., Prat-Pradal, D., Labat, J.-J., et al. (1998). Anatomical basis of pudendal nerve entrapment.
- Stecco, A., & Stecco, C. (2024). Fascial densification and neuropathic pain: clinical implications.
- Cholewa, J., et al. (2024). Myofascial entrapment in the Alcock’s canal: the role of pelvic floor hypertonia.
- Blue Portance — SBNFA™ Model. (2026). NEURO-ANATOMY — Part IV: Diagnostic wandering and chronicization.