

Diagnostic wandering and central sensitization in pudendal neuralgia
In pudendal neuralgia, the absence of objectifiable lesions on imaging does not imply the absence of a pathological mechanism. Diagnostic wandering exposes the nervous system to prolonged nociceptive input, promoting protective hypertonia and, over time, central sensitization.
1. Diagnostic wandering and delayed recognition
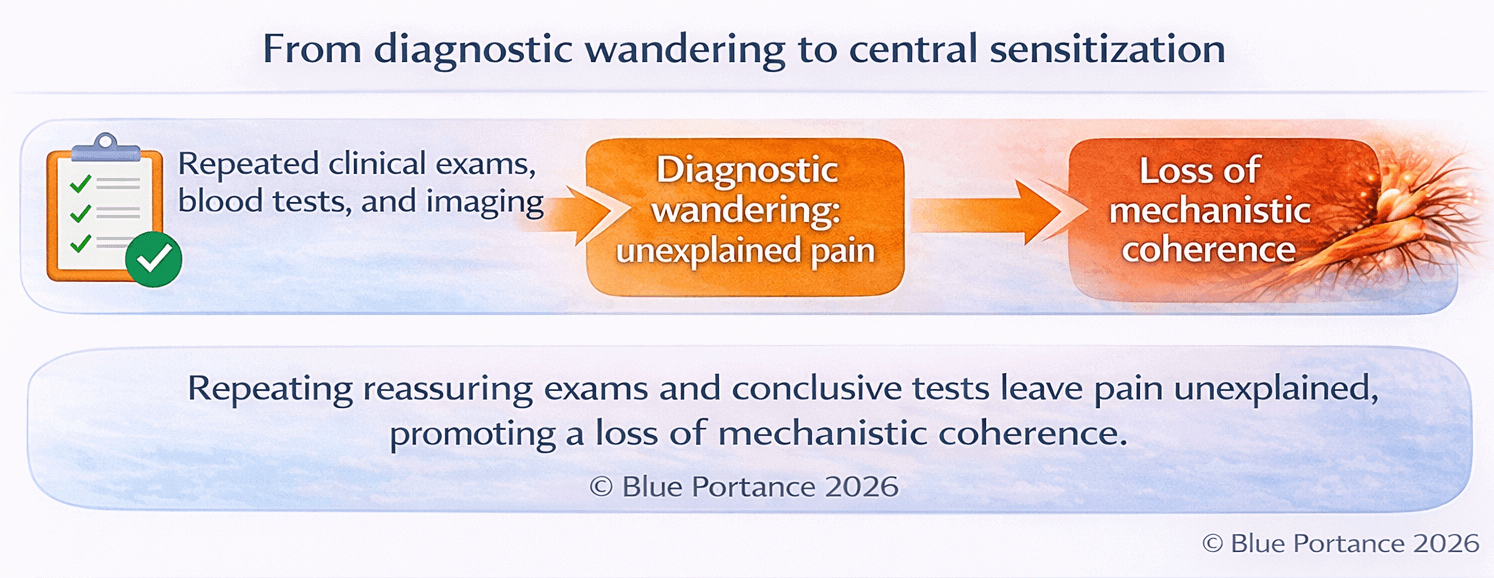
Pudendal neuralgia (PN) is associated with prolonged diagnostic delays, often extending over several years, due to low symptom specificity and the absence of consistent structural findings on imaging (Labat et al., 2008).
This diagnostic wandering is not merely an organizational delay. It exposes the nervous system to repeated nociceptive stimulation without a coherent mechanistic explanation, promoting unfavorable neurophysiological adaptations (FitzGerald et al., 2014).
© Blue Portance 2026
2. Referred pain and false organ diagnoses
Pain in PN is frequently interpreted as urological, gynecological, or anorectal in origin due to its perineal, urethral, or rectal localization. Yet these territories correspond to innervation zones of the pudendal nerve and its terminal branches (Labat et al., 2008).
Biological and morphological investigations are often normal. This discrepancy between severe symptoms and reassuring test results leads to multiple alternative hypotheses and inappropriate treatments, without addressing the underlying neuropathic mechanism (FitzGerald et al., 2014).
3. Medical invalidation and neuro-affective load
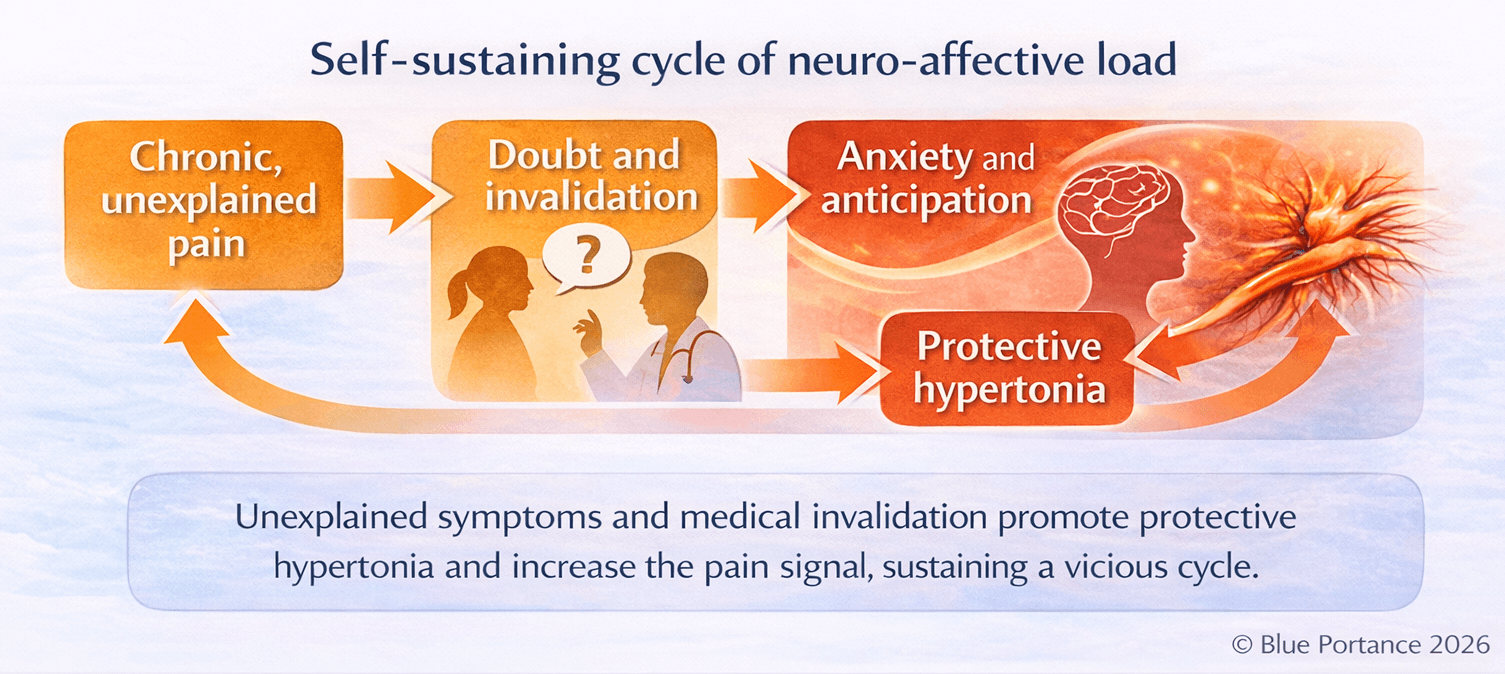
The absence of objective findings promotes medical invalidation—explicit or implicit— which alters the therapeutic relationship and the patient’s lived experience. This invalidation is a chronic stress factor, known to amplify pain perception and reinforce protective muscular responses (Linton & Shaw, 2011).
In chronic pelvic pain, this neuro-affective load is frequently associated with reflex pelvic hypertonia and pain anticipation, sustaining the vicious circle of pain (Darnall et al., 2017).
© Blue Portance 2026
4. Central sensitization and allodynia
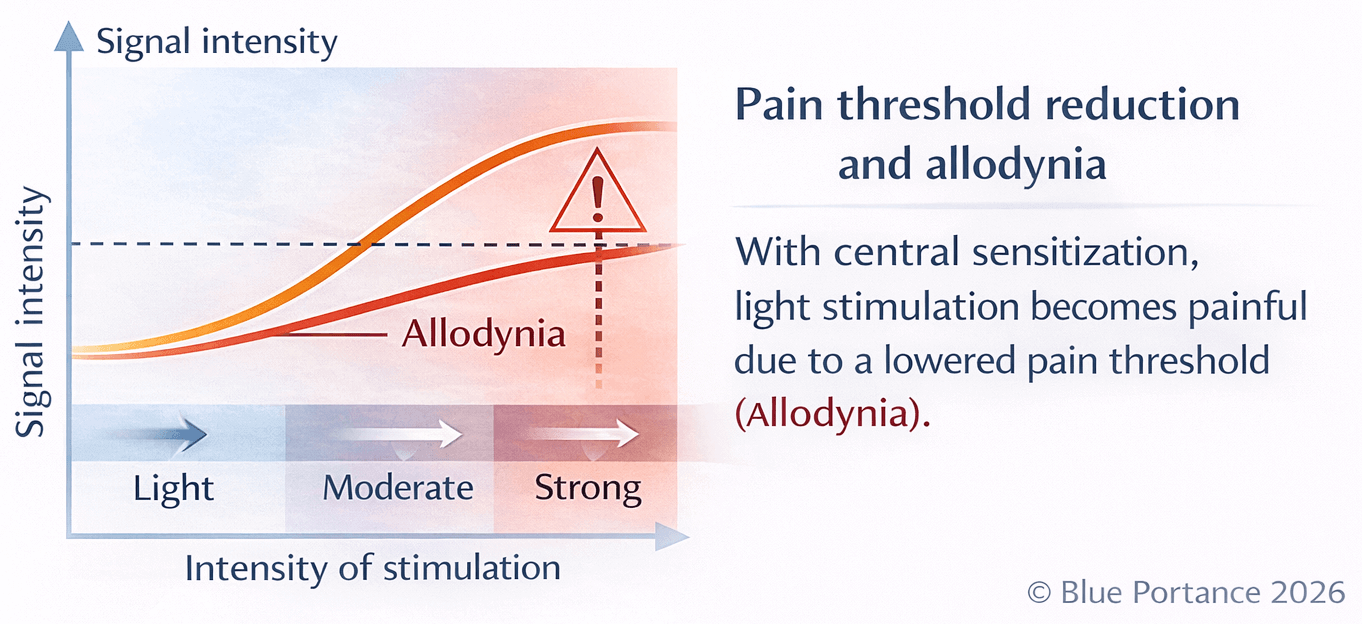
Central sensitization refers to a state in which the central nervous system amplifies nociceptive signals and lowers the pain activation threshold (Woolf, 2011).
In this context, normally non-painful stimuli—cutaneous contact, light pressure, clothing friction—may trigger intense pain: this is allodynia (Clauw, 2015).
Chronic pelvic pain conditions, including PN, show a strong propensity toward central sensitization, particularly when the diagnostic phase is prolonged and pain remains unexplained (FitzGerald et al., 2014; Nijs et al., 2014).
© Blue Portance 2026
5. Clinical implications for management
Recognizing central sensitization profoundly changes the therapeutic strategy. An exclusively local approach is often insufficient when central pain circuits are involved (Nijs et al., 2014).
Management therefore needs to reduce nervous system hypervigilance, restore mechanical variability, and provide the patient with a coherent understanding of symptoms—an essential condition for exiting diagnostic wandering and limiting chronicization (Clauw, 2015).
- Labat J.J., Riant T., Robert R., et al. (2008). Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment. Neurourology and Urodynamics, 27(4), 306–310.
- FitzGerald M.P., Koch D., Senka J. (2014). Centralized pain and chronic pelvic pain. American Journal of Obstetrics and Gynecology, 210(6), 545–552.
- Woolf C.J. (2011). Central sensitization: implications for the diagnosis and treatment of pain. Pain, 152(3), S2–S15.
- Clauw D.J. (2015). Diagnosing and treating chronic musculoskeletal pain based on the concept of central sensitization. Best Practice & Research Clinical Rheumatology, 29(1), 1–13.
- Nijs J., Meeus M., van Oosterwijck J., et al. (2014). Treatment of central sensitization in patients with chronic pain. Pain Physician, 17(3), 209–223.
- Linton S.J., Shaw W.S. (2011). Impact of psychological factors in the experience of pain. Physical Therapy, 91(5), 700–711.
- Darnall B.D., Carr D.B., Schatman M.E. (2017). Pain psychology and centralized pain. Physical Medicine and Rehabilitation Clinics of North America, 28(2), 301–315.