

Pain That Does Not Behave as Expected
One of the major challenges of coccydynia (tailbone pain) is distinguishing local pain from tailbone referred pain, because symptoms do not always behave as expected.
In some patients, it is obvious, precise, almost self-explanatory. In others, it disguises itself, shifts, radiates — to the point of casting doubt on the diagnosis.
Understanding the distinction between local pain and referred pain is essential, because this is often where diagnostic errors… and medical wandering begin.
Local Pain: A Precise Mechanical Signal
In its most typical form, coccydynia presents as strictly localized pain at the level of the coccyx.
The patient can often:
- point to the exact spot with a finger,
- describe pain triggered by direct pressure,
- clearly identify aggravating situations.
This pain is classically:
- worsened while sitting,
- exacerbated when transitioning from sitting to standing,
- sometimes triggered during defecation or certain pelvic movements [1] (Fogel et al., 2004).
“As long as I’m not sitting, I’m fine. But the moment I put pressure there, it feels like something is stabbing inside.”
This type of description is highly suggestive of direct mechanical involvement of the coccyx: dislocation, hypermobility, or local soft tissue irritation.
Clinically, reproducing the pain on coccygeal palpation constitutes a strong diagnostic argument, especially when it fits within a coherent mechanical context [1] (Fogel et al., 2004).
When Pain Travels: Understanding Tailbone Referred Pain
In other cases, the pain seems to originate elsewhere. This pattern of tailbone referred pain often leads to diagnostic confusion.
The patient may describe:
- diffuse perineal discomfort,
- pain in the buttocks,
- a burning or anterior pressure sensation,
- sometimes even pain resembling low sciatica.
👉 And yet, the origin often remains the coccyx.
This situation is confusing for both patient and practitioner. It explains why coccydynia is frequently mistaken for:
- a lumbar spine disorder,
- ano-rectal pain,
- a functional perineal disorder,
- or vaguely defined “nerve pain” [2] (Nathan et al., 2010).
Why the Coccyx Can “Send” Pain Elsewhere
To understand this phenomenon, we must abandon the idea of a compartmentalized body.
The sacrococcygeal region is a dense anatomical crossroads where intersect:
- bony structures,
- ligaments,
- pelvic floor muscles,
- closely interconnected nerve networks.
The coccyx is innervated by branches from the sacral and coccygeal plexuses and is functionally connected to structures such as the ganglion impar, located anterior to the sacrum [2] (Nathan et al., 2010).
When a mechanical structure is chronically irritated — for example, a hypermobile coccyx or one bearing a bone spur — pain may:
- be perceived at a distance,
- travel through shared neural pathways,
- manifest in neighboring areas sharing the same innervation territory [2] (Nathan et al., 2010).
It is similar to a splinter under the skin: the entry point is tiny, but the pain seems to spread far beyond.
Typical Clinical Example: When the Diagnosis Misses the Target
A patient consults for burning perineal pain aggravated by sitting. Urinary and digestive examinations are normal. The pain resists local treatments.
Only after careful clinical examination and appropriate imaging does one discover:
- coccygeal hypermobility,
- or a bone spur irritating the soft tissues.
👉 The pain was not “in the perineum” :
it was referred from the coccyx.
This situation is well described in clinical reviews, and explains why coccydynia can take very different forms depending on the patient [2] (Nathan et al., 2010).
This confusion is further amplified by a well-known phenomenon in modern neuroscience: central sensitization [3] (Sandrasegaram et al., 2020).
When coccygeal mechanics remain disturbed over a long period, the nervous system may enter a state of “high alert.” The pain threshold decreases globally.
This phenomenon, called central sensitization, means the brain may continue generating a pain signal even if the initial lesion has begun to stabilize [3] (Sandrasegaram et al., 2020).
In this context, pain may extend beyond its initial zone and radiate toward pudendal nerve or cluneal nerve territories, producing burning or electric sensations throughout the perineal region [3] (Sandrasegaram et al., 2020).
The challenge is no longer only to treat the bony “hinge,” but to calm a neurological alarm system that has become hypersensitive [4] (Dunkley & Brotto, 2016).
Why This Distinction Changes Everything
Confusing local tailbone pain and referred tailbone pain leads to two common errors:
- treating only the apparent painful area,
- ignoring the underlying mechanical mechanism.
Under these conditions, treatments are often:
- ineffective,
- partially effective,
- or effective… but only temporarily.
👉 Understanding where pain truly comes from makes it possible to stop chasing its manifestations.
Figure — Local vs Referred Pain in Coccydynia
📌 Figure — Local vs Referred Pain in Coccydynia
Recommended educational placement here
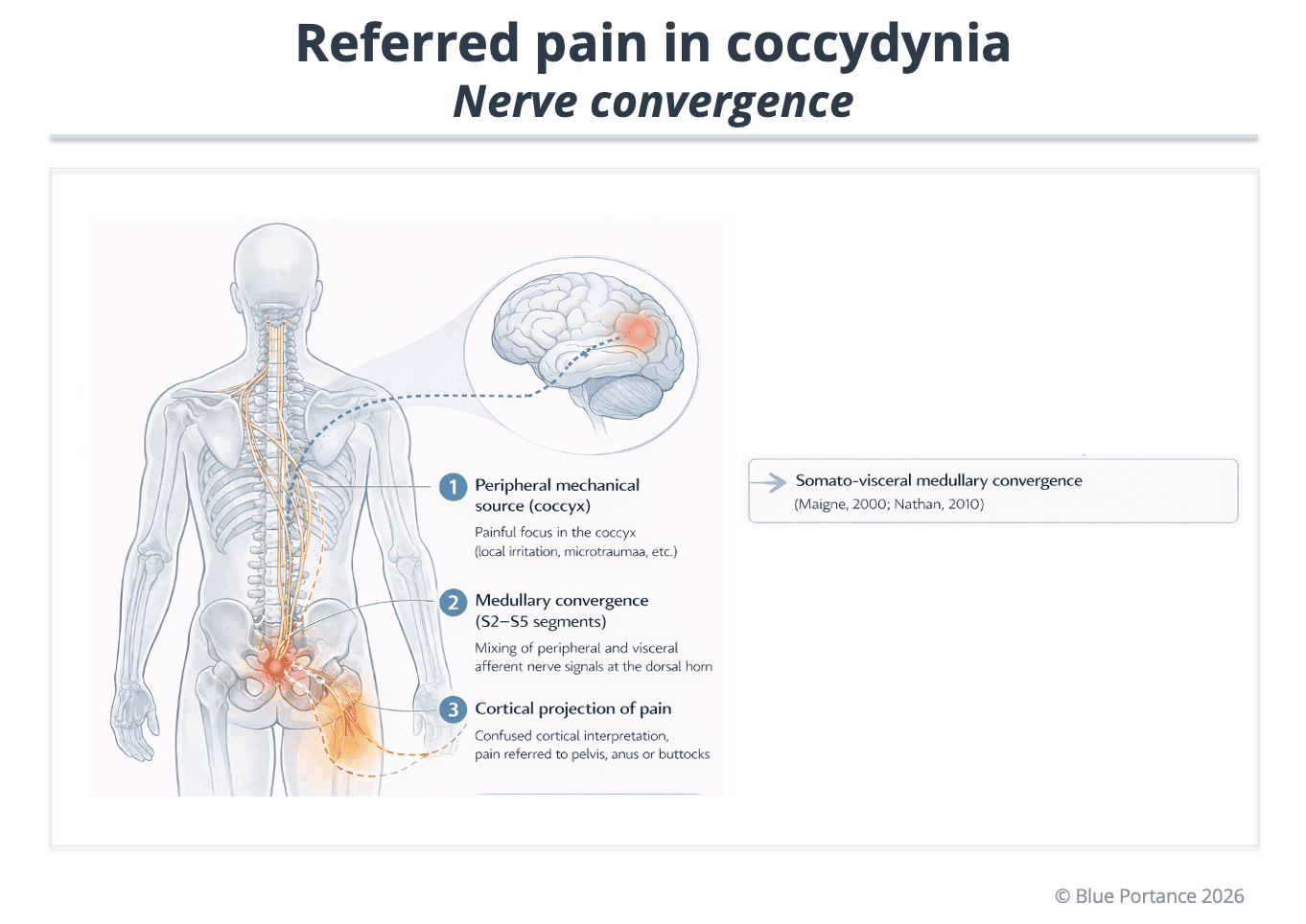
Referred pain in coccydynia follows the principle of segmental spinal convergence.
The coccyx is primarily innervated by sacral roots S2 to S5. Nociceptive afferents originating from the coccyx converge in the dorsal horn of the corresponding sacral segments.
This convergence can associate signals coming from:
- coccygeal osteo-ligamentous structures
- the pelvic floor
- perineal tissues
- certain pelvic visceral structures
Cortical interpretation of these signals generally remains confined to territories corresponding to the sacral dermatomes.
Referred pain may therefore be felt toward:
- the perineum
- the anus
- the buttocks
- the posterior thigh
- sometimes the low lumbar region
By contrast, radiation toward the neck or shoulder does not reflect a direct S2–S5 segmental projection. It would correspond to a different mechanism (global postural compensation, central sensitization, or another supra-segmental process).
- Fogel, G. R., Cunningham, P. Y., & Esses, S. I. (2004). Coccydynia: Evaluation and management. Journal of the American Academy of Orthopaedic Surgeons, 12(1), 49–54.
- Nathan, S. T., Fisher, B. E., & Roberts, C. S. (2010). Coccydynia: A review of pathoanatomy, aetiology, treatment, and outcome. Journal of Bone and Joint Surgery (British Volume), 92-B(12), 1622–1627.
- Sandrasegaram, S., Ramaraju, S., & Narayanan, R. (2020). Chronic pelvic pain and central sensitization. Journal of Pelvic, Obstetric and Gynaecological Physiotherapy, 126, 23–31.
- Dunkley, C. R., & Brotto, L. A. (2016). Psychological treatments for chronic pelvic pain. Clinical Obstetrics and Gynecology, 59(3), 558–571.