

1. Why There Is No Single Treatment for Coccydynia
(and why this is reassuring, not discouraging)
Chronic tailbone pain is one of the most challenging forms of coccydynia, because the mechanisms that sustain it are often misunderstood.
When pain persists, the question inevitably comes back:
“What do we do to make it stop?”
In coccydynia (tailbone pain), this question is often asked too early — or rather, asked without the problem being properly formulated.
Coccydynia is not a disease in the strict sense.
It is a pain syndrome, meaning the final clinical expression of different mechanisms
that can lead to the same symptom: pain while sitting.
Treating coccydynia as a single entity is like trying to repair a breakdown without knowing whether the problem comes from:
- a broken part,
- excessive play,
- mechanical jamming,
- or a global imbalance of the system.
This is precisely why there is no — and cannot be — a universal treatment.
2. What Clinical Literature Shows
Major clinical reviews converge on one fundamental point:
the effectiveness of care depends directly on understanding the dominant mechanism.
Fogel et al. (2004) highlight that treatment failures are often linked to overly generic approaches, applied without distinguishing between:
- structural forms of coccydynia,
- functional forms,
- mixed forms — the most common in real-world practice.
Lirette et al. (2014) emphasize that most patients improve when the strategy matches the mechanism, rather than when a standard treatment is applied indiscriminately.
👉 In other words:
the problem is not a lack of solutions,
but the mismatch between the cause and the response.
This diagnostic precision is even more crucial because some forms of coccydynia involve pain mechanisms often described as nociplastic.
Modern literature increasingly distinguishes purely mechanical pain from pain linked to nervous system sensitization (Nathan et al., 2010).
In these cases, even if the initial cause (a fall or childbirth) has resolved, the nervous system continues to emit an alarm signal. The approach then needs to become multidisciplinary.
For example, coccygeal hypermobility documented on dynamic radiographs may require local injections or stabilization, while pain without structural abnormality is more likely to benefit from pelvic floor rehabilitation aimed at relaxing the levator ani muscles (Fogel et al., 2004).
Trying to treat bony instability with relaxation — or muscular contracture with surgery — explains many of the failures observed along care pathways (Sandrasegaram et al., 2020).
3. Why Symptom-Based Approaches Often Disappoint
When facing chronic tailbone pain, the temptation is strong to silence it quickly: analgesics, imposed postures, rigid seating, generic advice…
These approaches may provide temporary relief, but they often fail in the medium term, because they do not change the mechanism that maintains the constraint.
In mechanical coccydynia, pain is not isolated inflammation.
It is the signal of a system that can no longer distribute loads properly.
- mask the alarm,
- leave the constraint intact,
- and expose the patient to recurrence.
4. A Logical Hierarchy, Not a Recipe
Management must be progressive, structured, and individualized.
- identify whether the problem is structural, functional, or mixed,
- identify patient-specific aggravating factors,
- adapt the strategy accordingly.
Maigne et al. (2000) show that certain mechanical abnormalities benefit from highly specific care, while others rely more on restoring mobility and adaptability.
👉 Searching for “the right treatment” without this prior step is like searching for a key… without knowing which door to open.
5. Why This Perspective Changes the Patient Experience
The absence of a simple answer is often experienced as abandonment. In reality, the absence of a single solution means there are multiple possible levers.
Understanding chronic tailbone pain helps patients move from frustration toward structured, mechanism-based care.
Time-to-care is a major prognostic factor. After several months, pain memory phenomena may develop (Dunkley & Brotto, 2016).
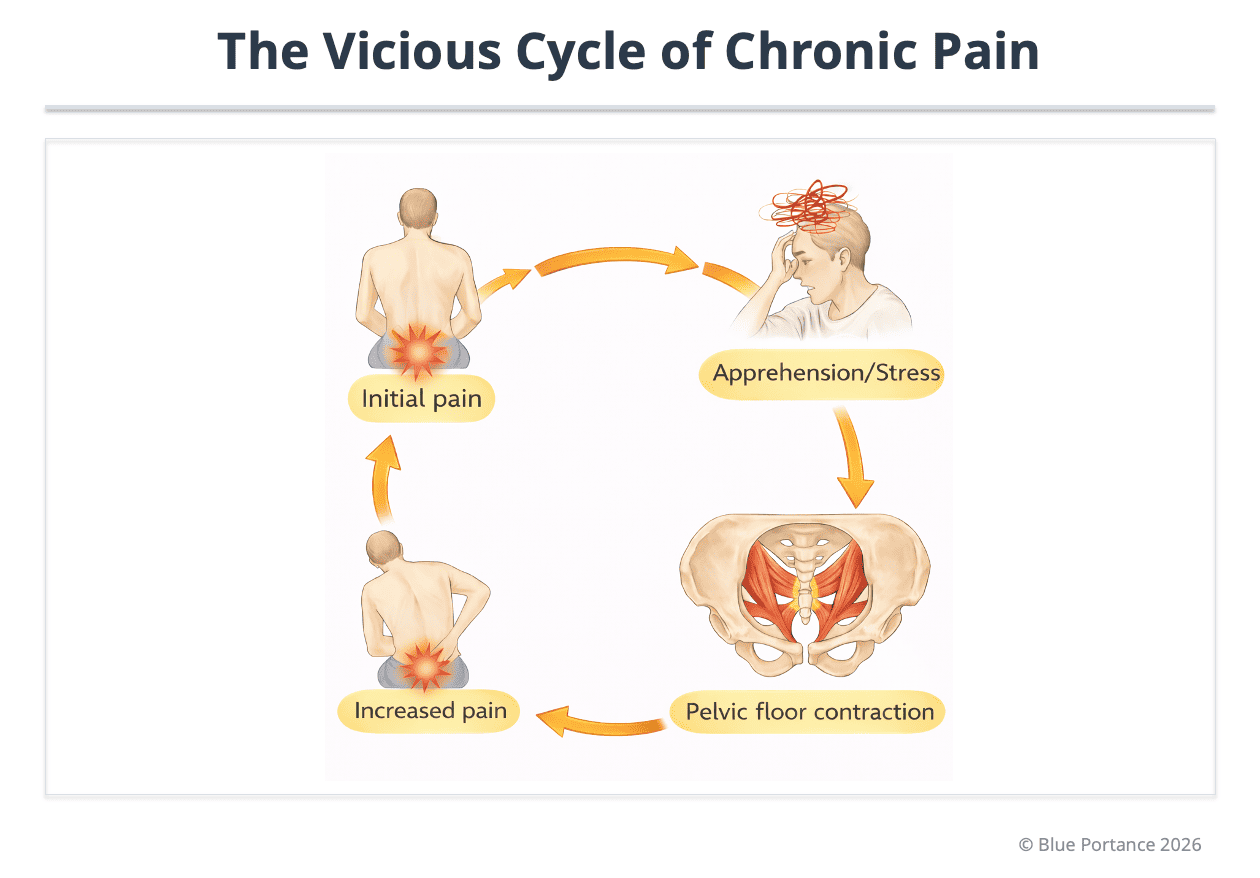
Fear of pain can trigger reflex pelvic floor contraction, which maintains coccygeal compression and fuels the vicious cycle (Lirette et al., 2014).
6. What This Article Does… and Does Not Do
This article does not propose a universal solution. It proposes a reading framework.
Understanding that there is no single treatment is not an admission of powerlessness. It recognizes that coccydynia is the endpoint of different mechanisms that require a response consistent with their own logic.
Before trying to eliminate pain, one must identify the mechanism that maintains it: mechanical instability, myofascial stiffening, postural maladaptation, or chronicity processes.
👉 This shift in perspective transforms the question “What should be done?” into a more fertile one: “What, in this specific case, maintains the constraint?”
- Fogel GR, Cunningham PY, Esses SI. Coccydynia: evaluation and management. J Am Acad Orthop Surg. 2004.
- Lirette LS et al. Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner J. 2014.
- Nathan ST et al. Coccygodynia: a review of pathoanatomy, aetiology, treatment, and outcome. J Bone Joint Surg Br. 2010.
- Sandrasegaram S et al. Imaging and management of coccydynia. Skeletal Radiology. 2020.
- Dunkley CR, Brotto LA. Psychological treatments for chronic pelvic pain. Clin Obstet Gynecol. 2016.
- Maigne JY et al. Results of coccygectomy for coccydynia. Spine. 2000.