

Introduction — “It feels like I’m sitting on a nail”
“When I sit down, it’s still manageable. But after a few minutes, a deep pain appears — as if something is pushing inward. And when I stand up, it’s like an electric shock.”
This description is strikingly consistent in individuals with coccydynia. The pain is rarely diffuse. It is precise, midline, often described as a nail or knife-like stab, sometimes a deep burning sensation at the terminal end of the spine (Nathan, Fisher & Roberts, 2010).
Over time, sitting becomes uncomfortable and then painful. Compensatory strategies appear: leaning to one side, shifting constantly, flexing forward, standing up early. Ordinary activities — desk work, driving, watching a movie — become persistent mechanical stressors (Nathan, Fisher & Roberts, 2010).
Despite this specific presentation, coccydynia is frequently misidentified. It may be confused with low back pain, sciatica, anorectal or perineal pain, or dismissed when static imaging appears normal (Nathan, Fisher & Roberts, 2010).
In most cases, however, coccydynia involves identifiable anatomical, biomechanical and neuro-functional mechanisms — provided the appropriate interpretive framework is applied.
1. A small bone with major functional impact
The coccyx forms the terminal segment of the vertebral column. It consists of three to five segments with variable fusion patterns (Woon & Stringer, 2012).
Although often considered vestigial, this interpretation is inaccurate. The coccyx serves as:
- an inferior anchoring point for major pelvic floor muscles (Standring, 2021; Vodušek, 2004),
- a contributor to pelvic ring stability (Standring, 2021),
- a direct interface between spine, pelvis and the seated support surface (Woon & Stringer, 2012).
It therefore functions as a mechanical cohesion node within a load-bearing structure, particularly in sitting (Nathan, Fisher & Roberts, 2010).
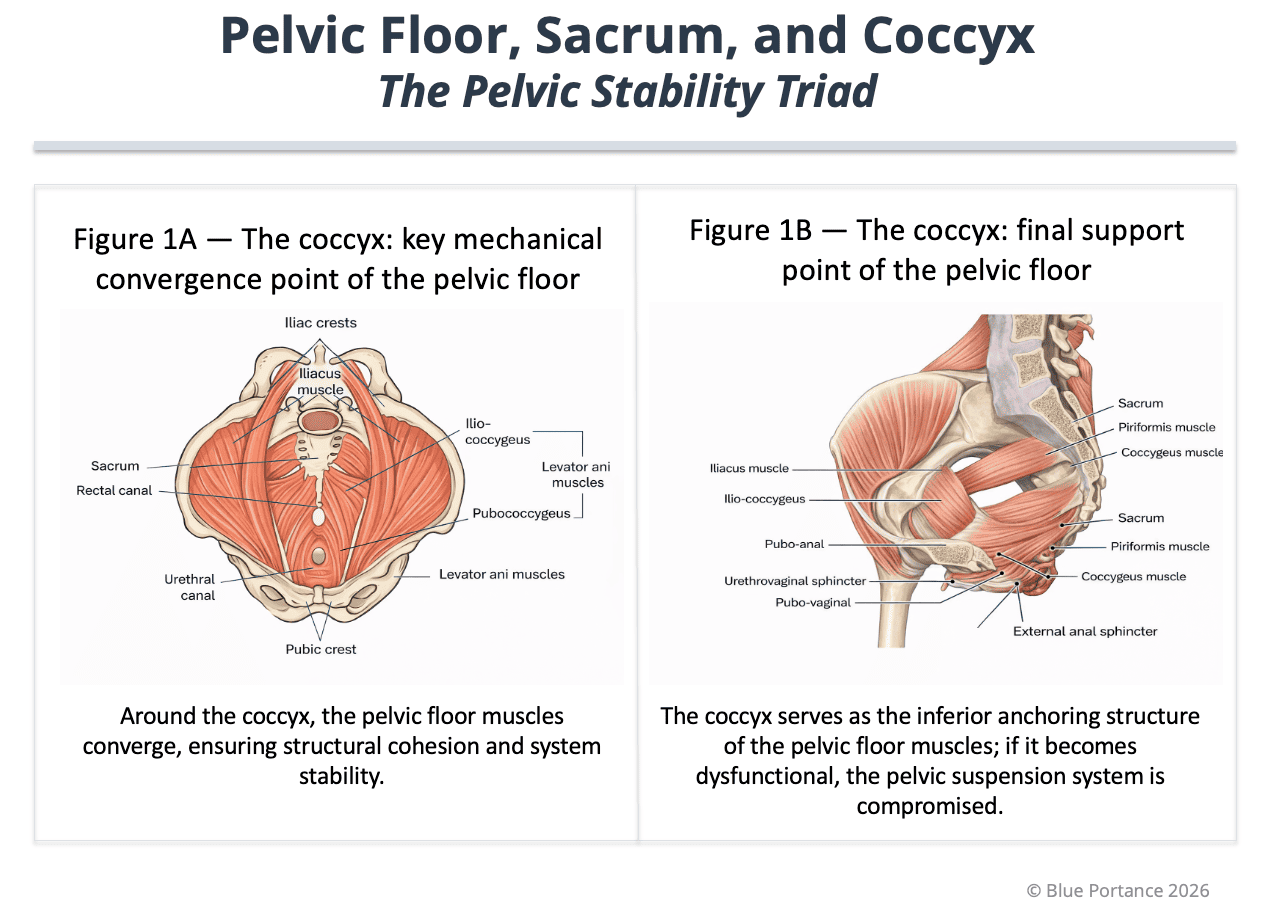
2. The coccyx as a pelvic floor support structure
The coccyx acts as an inferior convergence point for the pelvic floor. The posterior fibers of the levator ani and the coccygeus muscle insert in this region (Standring, 2021; Vodušek, 2004).
Through these attachments, the coccyx plays an active structural role, enabling coordinated tensioning of the pelvic sling and contributing to global pelvic stability and spinal-pelvic continuity (Standring, 2021; Vodušek, 2004).
When its mobility or alignment is altered, pelvic tension patterns may become disorganized, increasing local mechanical stress (Nathan, Fisher & Roberts, 2010).
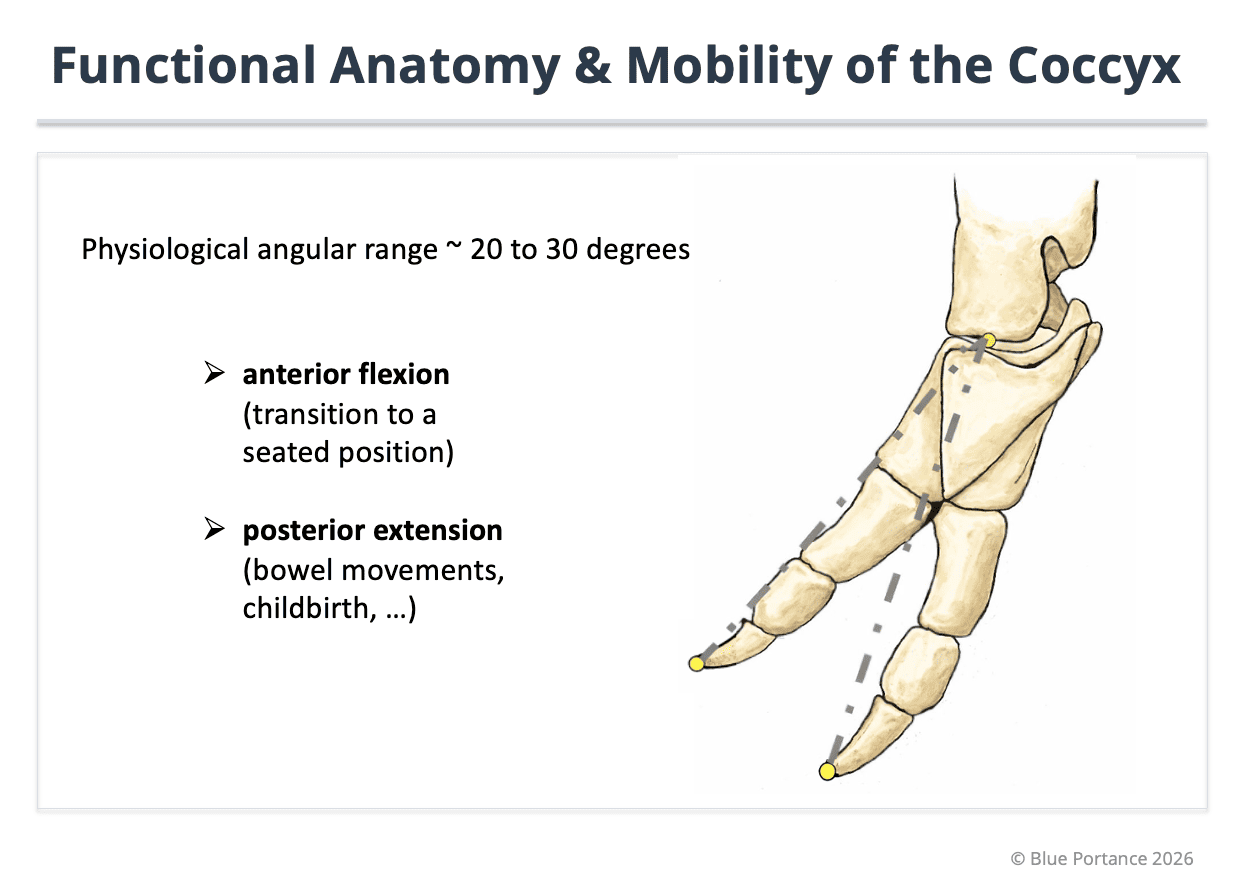
3. Biomechanics: essential intrinsic mobility
Contrary to common belief, the coccyx is not completely fixed. It demonstrates limited but functional mobility, especially during sitting, defecation and childbirth (Woon & Stringer, 2012; Nathan, Fisher & Roberts, 2010).
This mobility allows fine adaptation of pelvic geometry and prevents focal pressure concentration (Maigne, Doursounian & Chatellier, 2000).
- Excessive mobility (hypermobility or subluxation)
- Restricted mobility preventing adaptation
Static imaging may appear normal while dynamic load reveals dysfunction (Maigne, Doursounian & Chatellier, 2000).
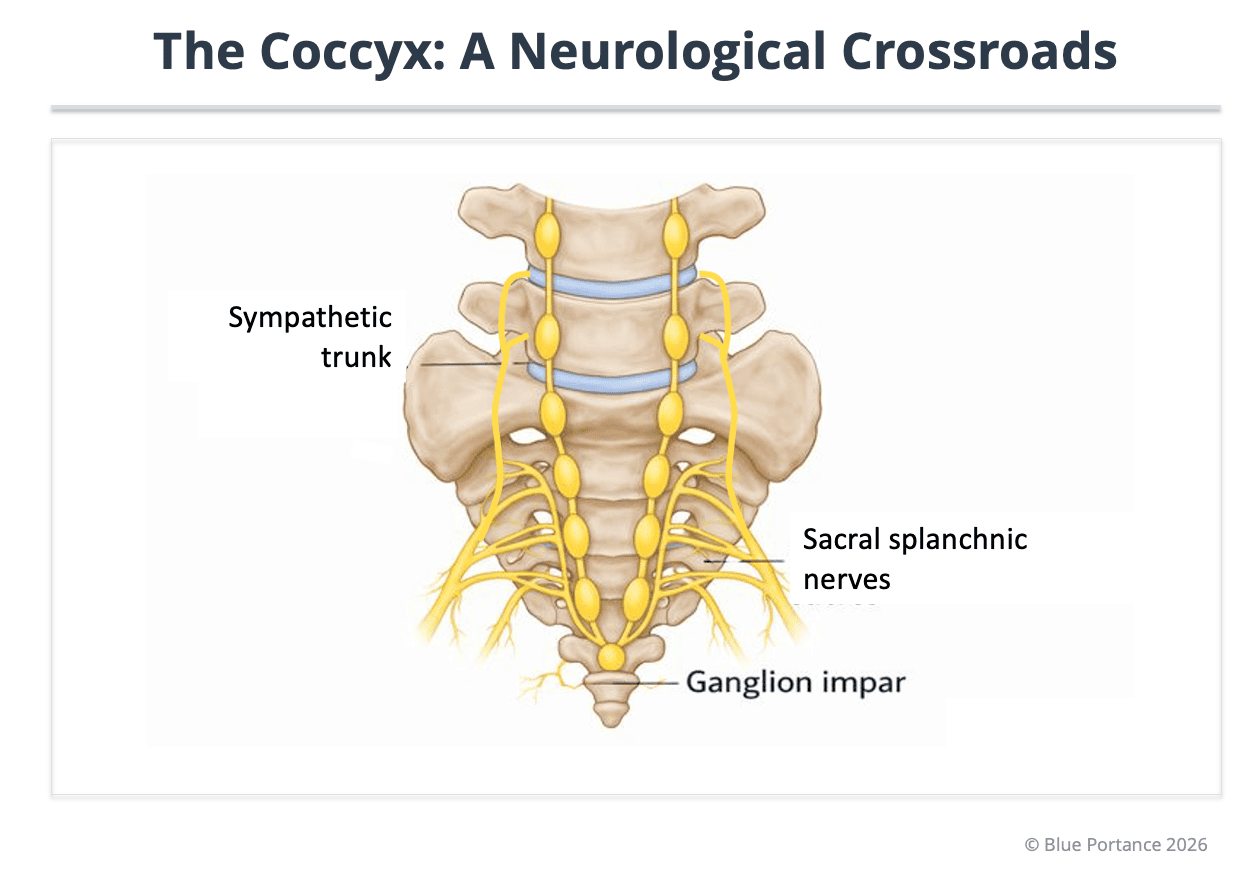
5. The coccyx as an inferior neurological crossroads
On its anterior surface lies the ganglion impar, the terminal convergence of the sympathetic chains. It plays a role in pelvic pain transmission and modulation (Sandrasegaram et al., 2020; Vodušek, 2004).
Chronic mechanical irritation may contribute to neurogenic sensitization, transforming localized mechanical dysfunction into persistent pain (Sandrasegaram et al., 2020).
Interim Conclusion
The coccyx cannot be reduced to a vestigial structure. It occupies a nodal position at the intersection of structural support, biomechanical adaptability and autonomic neurological modulation (Standring, 2021; Woon & Stringer, 2012).
Structural alteration or functional imbalance may lead to mechanical overload, pelvic instability and neurogenic sensitization (Maigne, Doursounian & Chatellier, 2000; Sandrasegaram et al., 2020).
- Postacchini, F. & Massobrio, M. (1983). Idiopathic coccygodynia: Analysis of fifty-one operative cases and a radiographic study of the normal coccyx. Journal of Bone and Joint Surgery (American Volume), 65(8), 1116–1124.
- Maigne, J.-Y., Doursounian, L. & Chatellier, G. (2000). Causes and mechanisms of common coccydynia: Role of body mass index and coccygeal trauma. Spine, 25(23), 3072–3079. doi: 10.1097/00007632-200012010-00015
- Woon, J. T. K. & Stringer, M. D. (2012). Clinical anatomy of the coccyx: A systematic review. Clinical Anatomy, 25(2), 158–167.
- Nathan, S. T., Fisher, B. E. & Roberts, C. S. (2010). Coccydynia: A review of pathoanatomy, aetiology, treatment and outcome. Journal of Bone and Joint Surgery (British Volume), 92-B(12), 1622–1627. doi: 10.1302/0301-620X.92B12.25486
- Standring, S. (ed.) (2021). Gray’s Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier.
- Sandrasegaram, N., et al. (2020). Diagnosis and management of sacrococcygeal pain. (Open-access article — PMC).
- Vodušek, D. B. (2004). Anatomy and neurocontrol of the pelvic floor. Digestion, 69(2), 87–92. doi: 10.1159/000077874
This chapter articulates (1) morphological patterns and structural lesions (Postacchini & Massobrio, 1983), (2) dynamic coccygeal mobility under load and clinical assessment (Maigne, Doursounian & Chatellier, 2000), and (3) precise anatomical attachments and pelvic floor support function (Woon & Stringer, 2012; Standring, 2021). The neurogenic dimension is framed by the anatomical reality of the ganglion impar and sympathetic pathways (Sandrasegaram et al., 2020) and pelvic neurocontrol physiology (Vodušek, 2004), without extrapolating a direct causal claim beyond available evidence.