

6. Coccyx morphology and mobility: multifactorial mechanical vulnerability
Coccydynia Knowledge Base
Coccyx morphology and mobility define how the tailbone adapts to sitting, movement, and mechanical stress. Variations in shape and dynamic behavior influence mechanical vulnerability in coccydynia (tailbone pain).
Coccyx morphology is neither uniform nor neutral across the general population. Anatomical and radiological data show substantial inter-individual variability, which shapes how mechanical loads from sitting, movement, and trauma are dissipated—or, conversely, concentrated.
This morphological diversity defines a baseline mechanical vulnerability: not pathological in itself and not systematically painful, but influential in how the system responds to environmental constraints.
1. The reference morphological classification
Foundational work by Postacchini and Massobrio (1983) proposed a morphological classification of the coccyx into four main types, based on curvature and orientation of coccygeal segments (Postacchini & Massobrio, 1983).
- Type I: coccyx slightly curved forward, harmoniously extending the sacrum.
- Type II: more marked ventral curvature, tip directed toward the pelvic cavity.
- Type III: abrupt anterior angulation between two segments.
- Type IV: subluxation or inter-segmental instability.
Identification of these types relies in particular on dynamic sitting/standing radiographs, as standardized by Maigne et al. (1996) (Maigne et al., 1996).
This approach showed a correlation between certain morphologies (II, III, IV) and a higher incidence of coccydynia, including in the absence of visible lesions on static imaging (Maigne et al., 1996 ; Nathan et al., 2010).
2. Anatomical predisposition and response to trauma
With comparable trauma—similar fall, similar childbirth, identical sitting constraints— some individuals develop persistent chronic pain, while others recover spontaneously.
Pain then appears as the encounter between:
- a specific bony architecture (morphological baseline), and
- a mechanical environmental constraint (sitting, repetition, impact),
- that the system can no longer absorb (adaptive dysfunction).
3. Toward an expanded morphological reading
Clinical data expanded the morphological reading toward six profiles, integrating retroverted or lateralized forms, and configurations associated with spicules (Nathan et al., 2010 ; Garg & Ahuja, 2021).
These morphotypes are not isolated causes. They should be read as mechanical vulnerability factors, whose expression depends on dynamic behavior.
- A morphotype is a constitutional anatomical configuration: inter-individual variation in curvature, angulation, or alignment. It defines a baseline, not a diagnosis.
- A lesion is an acquired and objective alteration: fracture, dislocation, unstable subluxation, post-traumatic instability.
- Without this distinction, a false conclusion becomes possible: “I have type III → I am ill.” The correct doctrine is: morphology defines a baseline; a lesion corresponds to a rupture of adaptive balance.
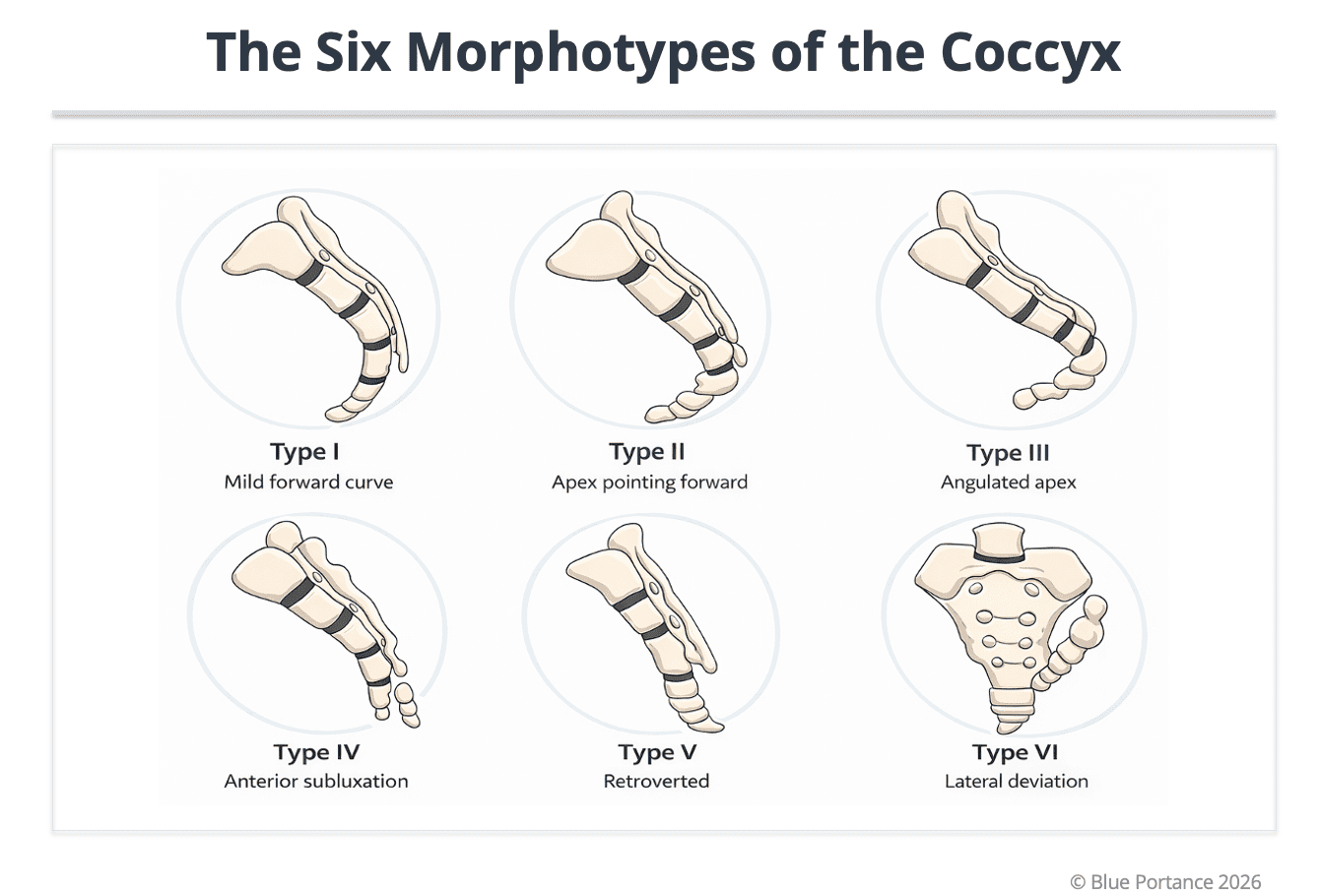
Morphological variations (types I to VI). Morphology defines a baseline mechanical vulnerability; clinical expression depends on dynamic mobility and sitting constraints (Postacchini & Massobrio, 1983 ; Maigne et al., 1996).
| Type | Anatomical description | Mechanical characteristics | Link with coccydynia |
|---|---|---|---|
| Type I | Gentle curvature, aligned with the sacrum | Good load dissipation | Low painful prevalence |
| Type II | Marked ventral curvature | Load concentration in sitting | Moderate to high prevalence |
| Type III | Anterior segmental angulation | Localized mechanical conflict point | High prevalence |
| Type IV | Sacro- or inter-coccygeal subluxation | Dynamic instability (sitting/standing) | Strongly associated with pain |
| Type V | Retroversion ± bony spicule | Chronic tissue irritation | Very strong association |
| Type VI | Lateral deviation / asymmetric alignment | Asymmetric loads | Atypical or referred pain |
These profiles are neither a diagnosis nor a fatality. They represent baseline mechanical vulnerability factors, whose clinical expression depends on coccyx morphology and mobility, soft-tissue status, and repeated mechanical constraints.
4. Segmental biomechanics: from morphotype to mechanical behavior
Talking about the coccyx “overall shape” helps with classification, but it is insufficient to understand mechanics.
The coccyx is a terminal hinge composed of 3 to 5 segments, linked by inter-coccygeal joints, and articulated with the sacrum (sacrococcygeal joint). Mechanics are therefore not monobloc.
Concretely, each morphotype influences:
- the location of the center of rotation dynamically,
- the existence of a segmental angulation point,
- the presence of a load concentration zone in sitting,
- and how forces are dissipated… or focused.
Key example: a type III is not simply “more curved.” It is a segmental angulation that can become a localized mechanical conflict point. A type IV adds a dimension of dynamic instability, generally better documented with functional imaging (sitting/standing) (Maigne et al., 1996).
- We no longer read only: “Here are the 6 shapes.”
- We read: “Here is how each architecture can behave dynamically.”
5. Physiological mobility: hypermobility vs hypomobility
The coccyx is not only a shape: it is a dynamic segment. Dynamic sitting/standing radiographs have shown physiological mobility, often described within a range of about 20 to 30 degrees depending on context, highlighting its role as a terminal shock absorber (Maigne et al., 1996).
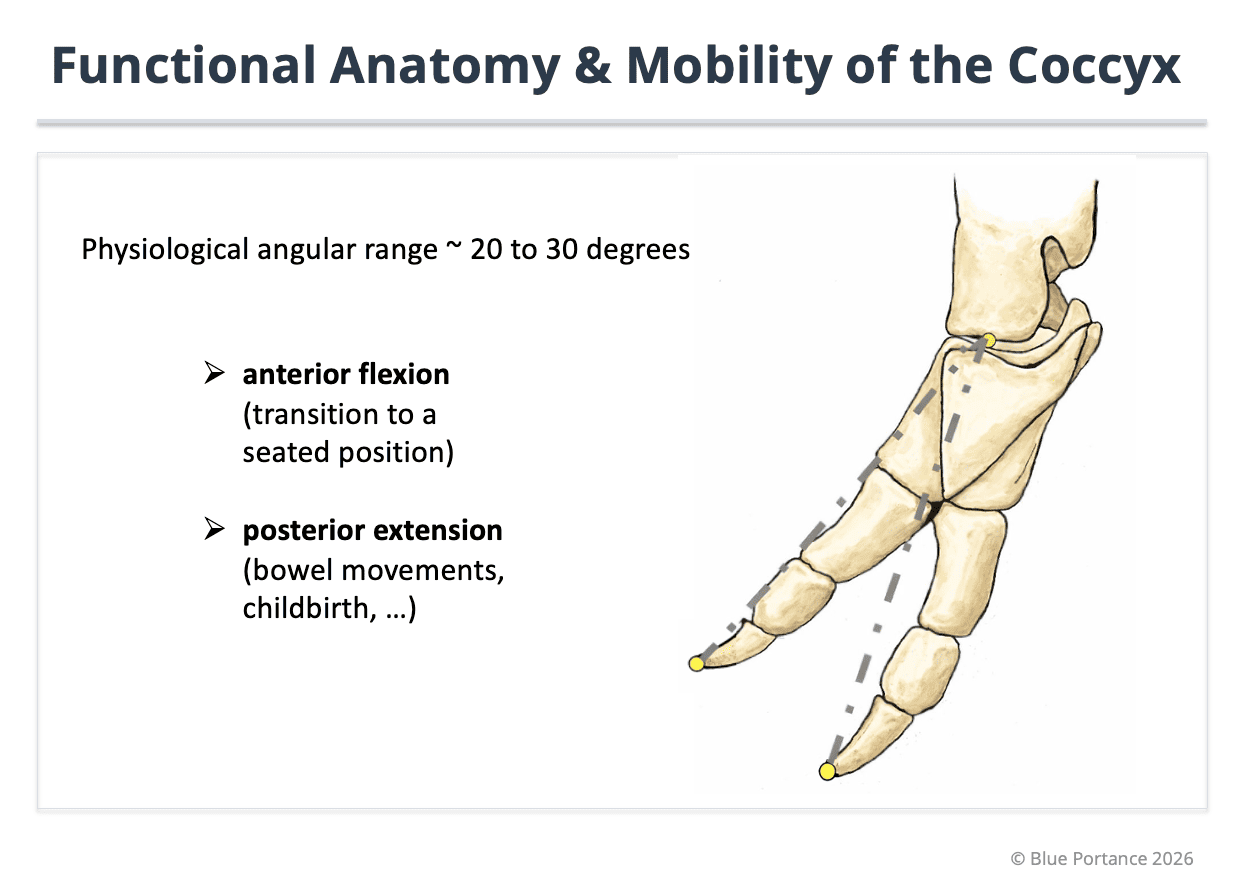
Illustration of normal flexion-extension angular range (about 20–30°) observed on dynamic sitting/standing imaging. The coccyx acts as an adaptive terminal hinge of the spine. Hypermobility (excess angulation) as well as hypomobility (stiffening) can impair load dissipation and promote abnormal load transmission toward soft tissues (Maigne et al., 1996).
Two opposite deviations can generate pain:
- Hypermobility: excessive angulation in sitting, segmental instability, repeated micro-trauma, local nociceptive activation — frequently described in patterns associated with types III–IV when unstable (Maigne et al., 1996 ; Nathan et al., 2010).
- Hypomobility: adaptive blocking, loss of terminal damping, more direct load transmission. Often less visible on static imaging, but clinically relevant (post-traumatic / protective stiffening).
Doctrinal consequence: the same morphology can be asymptomatic if it remains mobile, painful if it stiffens, and painful if it becomes unstable. Pain depends on the interaction: Morphology × Mobility × Environmental constraints.
Simple examples:
- Type II mobile → preserved damping; Type II stiff → load concentration.
- Type III stable → adaptation possible; Type III unstable → repeated micro-trauma.
- Types V–VI: retroversion / asymmetry → mechanical vectors that may increase tissue conflict or referred pain depending on context.
6. Interaction with soft tissues: the clinical “so what”
The coccyx is not an isolated bone. It sits at a crossroads of insertion and tension: pelvic floor, sacrotuberous ligament, gluteus maximus, posterior fascial convergence. Any variation in morphology or mobility changes tissue tensions.
In practice:
- If hypermobile: repeated ligament traction, irritation of muscular insertions, local micro-inflammation, peripheral sensitization.
- If hypomobile: loss of damping, compression of posterior tissues, loss of fascial glide, defensive pelvic floor hypertonicity.
In both cases, pain is not “purely bony”: it becomes myofascial and neuro-mechanical. Morphology does not directly cause pain; it changes how forces are transmitted to soft tissues, which can trigger local inflammation, reflex contraction, and a vicious pain cycle (Nathan et al., 2010 ; Garg & Ahuja, 2021).
Doctrinal conclusion
- Coccygeal morphology is neither a diagnosis nor a direct cause: it defines a mechanical baseline.
- Pain emerges from the interaction between bony architecture (morphotype), dynamic behavior (hyper/hypomobility), environmental constraints (sitting, trauma, repetition) and soft-tissue response (muscles, ligaments, fascia).
- Coccydynia is not only bony: it is a dynamic interaction between a terminal hinge and surrounding tissues.
- The clinical goal is to identify the dominant mechanism (instability, stiffening, tissue conflict) to guide evaluation and strategy.
- Postacchini F, Massobrio M. Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal coccyx. J Bone Joint Surg Am. 1983;65(8):1116–1124. PMID: 6619183
- Maigne JY, Tamalet B. Standardized radiologic protocol for the study of common coccygodynia and characteristics of the lesions observed in the sitting position. Spine (Phila Pa 1976). 1996;21(22):2588–2593. PMID: 8946914
- Maigne JY, Doursounian L, Chatellier G. Causes and mechanisms of common coccygodynia: role of body mass index and coccygeal trauma. Spine (Phila Pa 1976). 2000;25(23):3072–3079. PMID: 11145819
- Nathan ST, Fisher BE, Roberts CS. Coccygodynia: a review of pathoanatomy, aetiology, treatment, and outcome. J Bone Joint Surg Br. 2010;92(12):1622–1627. PMID: 21048171
- Garg B, Ahuja K. Coccydynia: imaging and management. J Clin Orthop Trauma. 2021. PMID: 33414167