

1. The Central Question
At this stage, one question becomes central in structural vs functional tailbone pain — and it determines everything that follows in coccydynia.
why does this coccyx hurt?
Is it because it is structurally injured?
Or because it is functionally trapped in an environment that no longer allows it to do its job?
Understanding structural vs functional tailbone pain helps clarify whether the issue lies in an objective mechanical lesion or in functional constraint.
This distinction may sound theoretical. In reality, it is fundamental, because it determines:
- which tests are actually useful,
- the logic of care,
- and above all, why some treatments fail while others work.
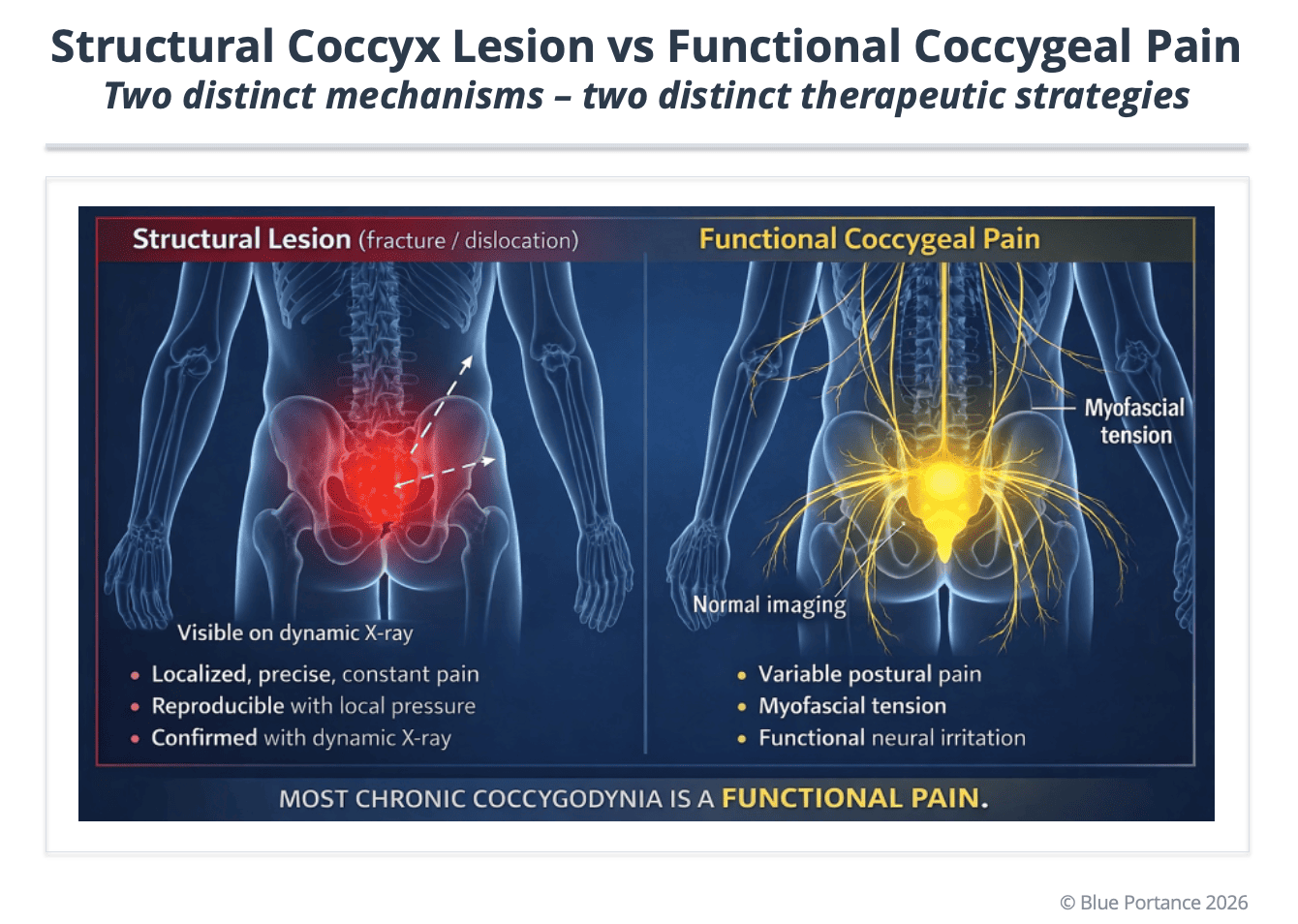
2. Structural Causes: When the Bone Is the Problem
In some cases of coccydynia, pain is linked to an objective abnormality of the coccyx itself.
The main findings are:
- an anterior or posterior dislocation (Postacchini & Massobrio, 1983; Maigne et al., 2000),
- an excessive hypermobility (Maigne et al., 1996; Lirette et al., 2014),
- more rarely a coccygeal bone spur (spicule) (Fogel et al., 2004; Lirette et al., 2014).
These abnormalities share an essential feature:
they are often invisible on a standard X-ray performed in standing or supine position.
This is precisely what led Maigne and colleagues to develop a sitting/standing dynamic X-ray protocol, now considered a reference approach in the workup of coccydynia (Maigne et al., 1996).
👉 What this dynamic imaging reveals is not only the shape of the coccyx, but how it behaves under load (Maigne et al., 1996; Lirette et al., 2014).
In many cases of structural vs functional tailbone pain, imaging alone does not provide the full explanation.
A coccyx may look perfectly normal at rest…
and dislocate, shift, or become hypermobile as soon as the patient sits (Maigne et al., 1996).
This is often the moment the diagnosis changes:
pain is no longer “unexplained”— it becomes mechanically coherent.
3. When Imaging Is Normal… but Pain Is Very Real
In a significant number of cases, imaging — even dynamic studies — reveals no obvious structural abnormality (Fogel et al., 2004; Lirette et al., 2014).
And yet, the pain is there.
Intense. Disabling.
This is where the concept of functional coccydynia comes in (Fogel et al., 2004).
In these situations, the coccyx is not injured, but it is trapped in an environment that has lost its capacity to adapt:
- pelvic floor hypertonicity (Vodusek, 2004),
- chronic muscle tension (Fogel et al., 2004),
- loss of overall pelvic mobility,
- repeated postural constraints.
The coccyx becomes the fixation point of a broader imbalance.
The bone is not “sick,”
the system around it can no longer absorb load.
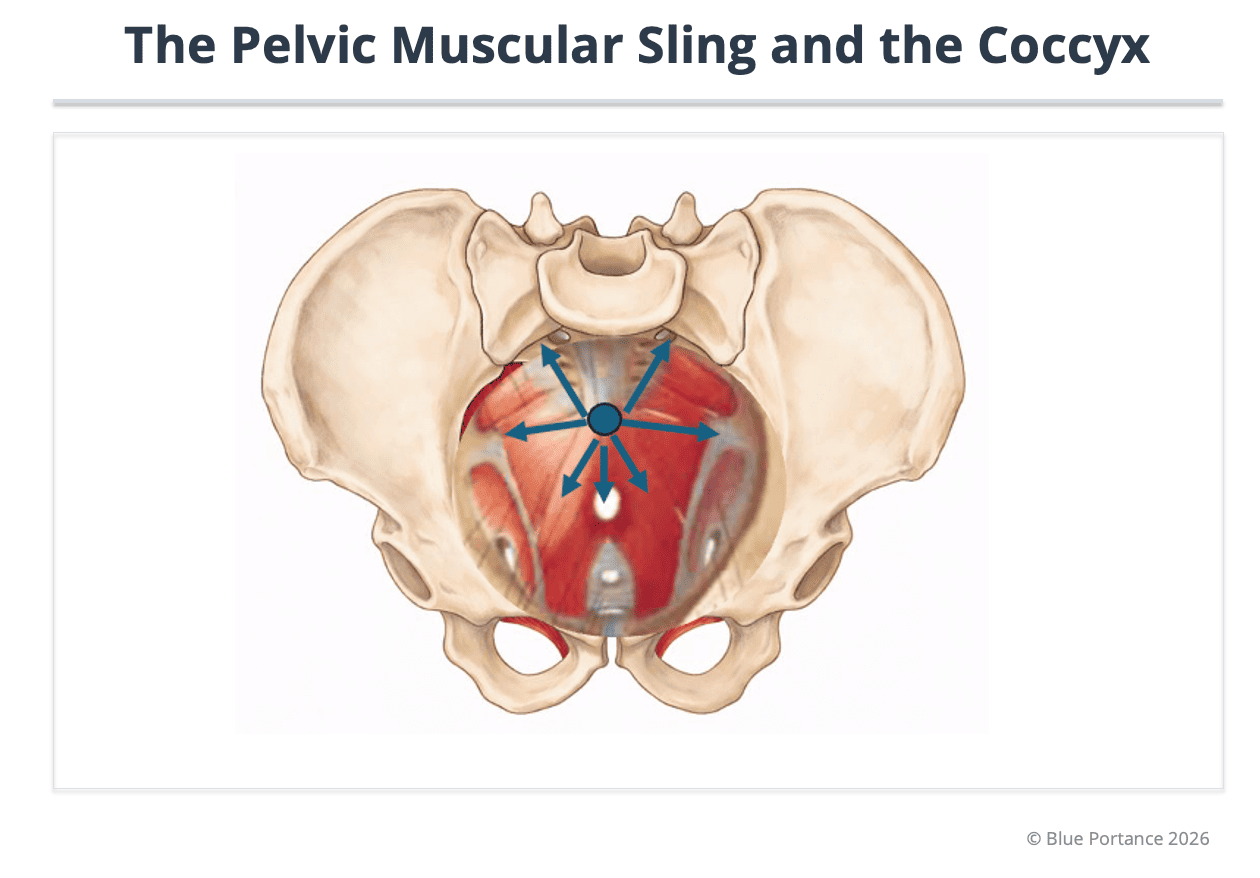
If imaging remains silent, the key is often found in the dynamics of the soft tissues that “guy” the coccyx.
Functional coccydynia often reflects pelvic floor hypertonicity.
The levator ani and coccygeus muscles insert directly along the lateral borders of the coccyx (Vodusek, 2004).
In chronic stress or a protective reflex after trauma, these muscles may enter a cycle of persistent contraction (Fogel et al., 2004).
The coccyx can then become “fixed” by overly tense muscular guy-wires, losing its ability to tilt during the transition into sitting (Fogel et al., 2004).
On clinical exam, reproducing pain by tensioning these muscles supports the idea that the bone is the victim of a myofascial environment that has become too rigid (Fogel et al., 2004).
This mechanism helps explain why some patients show no abnormality on Maigne’s dynamic radiographs, yet still experience a real mechanical constraint imposed by their own musculature (Maigne et al., 1996; Fogel et al., 2004).
4. The Key Role of the Clinical Exam
In these functional forms, the clinical examination becomes crucial.
Palpation helps to:
- reproduce the pain,
- assess coccygeal mobility,
- identify areas of muscular tension,
- detect protective responses of the pelvic floor.
A coccyx that is painful to palpation with normal imaging is not a “false problem.”
It often reflects local hypersensitization or an indirect mechanical constraint (Fogel et al., 2004).
👉 Again, pain makes sense.
It indicates a loss of functional freedom, not necessarily a visible lesion.
The “structural vs functional” distinction does not oppose “real” pain to “imaginary” pain. It contrasts an objective bony lesion or instability with an indirect mechanical constraint produced by the myofascial environment and postural dynamics.
When imaging is normal, the functional hypothesis becomes central: it requires looking for what “guy-wires” the coccyx (pelvic floor, tension, loss of mobility) and what prevents the system from absorbing load while sitting (Vodusek, 2004; Fogel et al., 2004).
In other words: the bone may be intact, but the system around it may have become too rigid to remain compatible with sitting load (Maigne et al., 1996; Lirette et al., 2014).
5. A Structuring Metaphor: A Healthy Part in a Jammed Mechanism
You can compare this situation to a mechanical part that is perfectly intact… but integrated into a jammed system.
- The part (the coccyx) is healthy.
- The surrounding axes (muscles, ligaments, posture) are rigid.
- Overall movement becomes constrained.
- The load concentrates on the most exposed point.
Pain is not proof of intrinsic fragility.
It is the signal of an imbalance in how loads are distributed.
6. Why This Distinction Prevents So Many Errors
Failing to distinguish structural from functional tailbone pain leads to two common dead ends:
- endlessly searching for a visible lesion that is not there,
- or, conversely, treating “functionally” a very real mechanical instability.
In both cases, the patient becomes exhausted, doubts, and ends up believing the pain is “in their head.”
👉 Yet, whether structural or functional, coccydynia is never imaginary.
It is always the expression of a system that can no longer adapt.
Purpose: to show why static imaging can be normal while mechanically coherent pain persists, and why clinical examination and functional interpretation remain decisive (Maigne et al., 1996).
- Maigne, J. Y., Pigeau, I., & Roger, B. (1996). Magnetic resonance imaging findings in the painful adult coccyx. European Spine Journal, 5(5), 333–336.
- Fogel, G. R., Cunningham, P. Y., & Esses, S. I. (2004). Coccydynia: Evaluation and management. Journal of the American Academy of Orthopaedic Surgeons, 12(1), 49–54.
- Vodusek, D. B. (2004). Pelvic floor neurophysiology. Clinical Neurophysiology, 115(6), 1329–1341.
- Postacchini, F., & Massobrio, M. (1983). Idiopathic coccygodynia. Journal of Bone and Joint Surgery, 65(8), 1116–1124.
- Maigne, J. Y., Doursounian, L., & Chatellier, G. (2000). Causes and mechanisms of common coccydynia: role of body mass index and coccygeal trauma. Spine, 25(23), 3072–3079.
- Lirette, L. S., Chaiban, G., Tolba, R., & Eissa, H. (2014). Coccydynia: An overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner Journal, 14(1), 84–87.