

1. Context and objectives
Pudendal neuralgia (PN) is not merely “perineal pain.” It corresponds to a progressive mechano-neuro-fascial maladaptation resulting from the interaction between pelvic geometry, posture, sitting-related constraints, pelvic floor tensions, and the intrinsic dynamics of the pudendal nerve.
When the system’s adaptive reserve is exceeded, compression, loss of neural gliding, fascial densification and protective hypertonicity may develop, leading to neuropathic pain that is often poorly localized (referred pain). This complexity explains the frequency of diagnostic wandering and the central role of central sensitization in chronic forms. Understanding these mechanisms helps orient clinical reasoning, avoid misleading hypotheses and structure a coherent approach integrating posture, sitting and rehabilitation.
In this context, the purpose of this knowledge base is to provide a rigorous and coherent explanatory foundation to understand pudendal neuralgia without reducing it to an isolated symptom (“urinary burning,” “rectal pain,” “genital hypersensitivity,” etc.). It aims to clearly distinguish causes, mechanisms and vulnerability factors, to move beyond frequent clinical confusion:
- pain can be intense without visible lesions,
- and conversely, an anatomical abnormality can exist without pain.
In pudendal neuralgia, the perceived location of pain does not necessarily indicate the origin of the conflict. Pain can be “referred” through neural convergence: you may feel pain in an area where the organ itself is healthy, while the mechanical constraint is located more proximally along the nerve pathway.
This knowledge base provides neither diagnosis nor medical treatment protocols. It offers a mechanistic reading framework that is essential to any coherent care pathway, and clarifies situations where a functional approach is relevant, versus those where structural involvement requires specialized evaluation.
2. Logical framework (reading key)
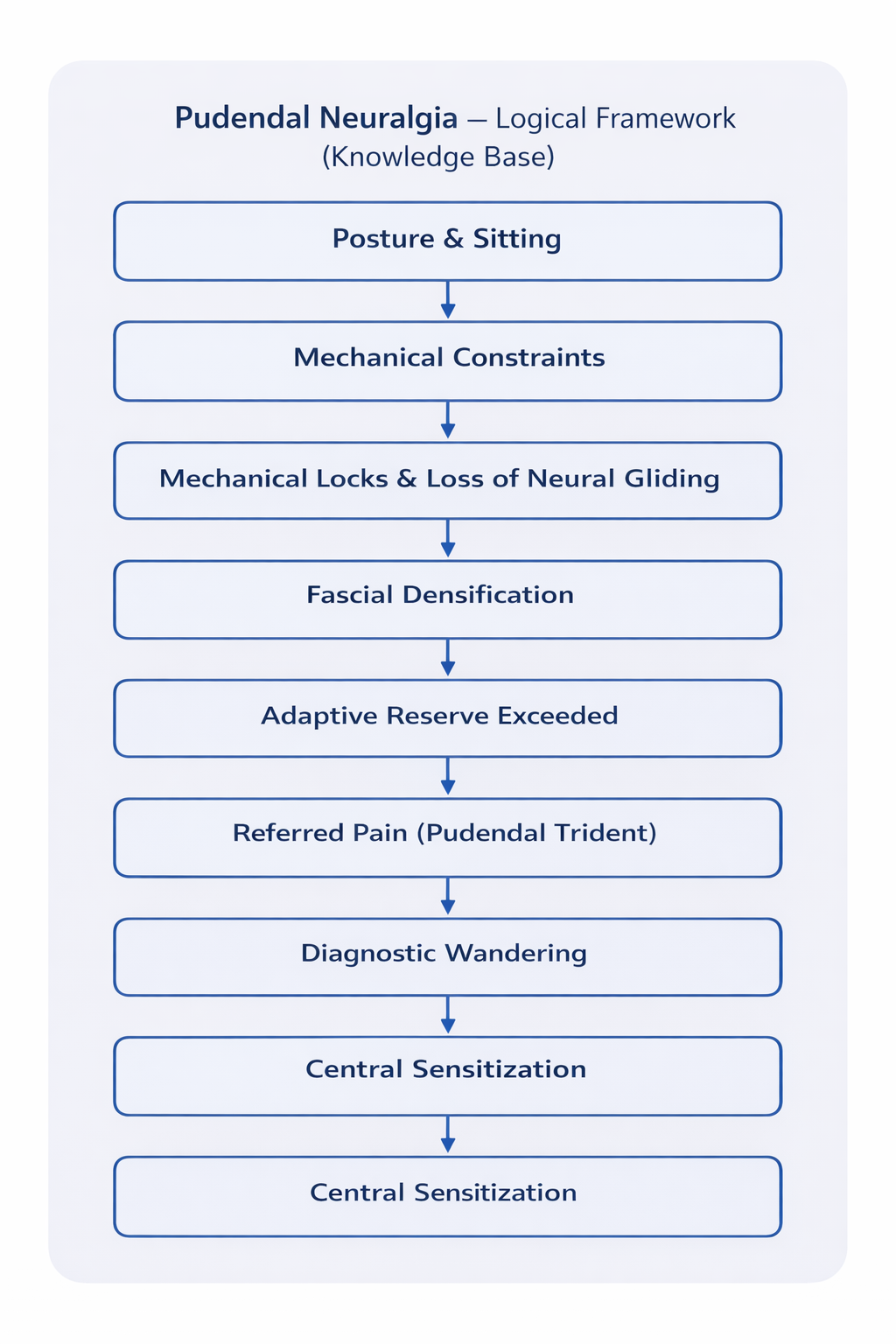
The diagram opposite provides a synthetic and operational view of the mechanisms described in this knowledge base.
It represents the progressive chain of maladaptation that can lead to pudendal neuralgia: starting from the interaction between posture and sitting, repeated mechanical constraints may generate mechanical locks and alter pudendal nerve gliding within its fascial interfaces.
Over time, the tissue environment of the nerve may densify, reducing its tolerance to mechanical stress. When the system’s adaptive reserve is exceeded, neuropathic pain appears, often poorly localized — referred pain following the pudendal “trident.”
This mechano-neuro-fascial complexity promotes diagnostic wandering. In chronic forms, central sensitization frequently develops, where the nervous system becomes hyper-reactive.
This diagram is not intended to replace the chapters: it is the compass and the red thread.
3. Recommended reading pathway
Understanding pudendal neuralgia follows a logical progression. Each page below is self-contained, yet integrated into a unified reasoning pathway (anatomy → locks → referred pain → triage → tissues → chronicization).
4. Access the chapters
5. How to use this knowledge base
- Read in order for a complete understanding (anatomy → mechanics → triage → tissues → chronicization).
- Go directly to a chapter depending on the question: posture and sitting, urinary burning “without infection,” rectal pain, etc.
- Compare structural vs functional before concluding on a single strategy: pudendal neuralgia is not one single disease, but a spectrum.
- Use this base as a reasoning framework: it does not replace medical advice and does not constitute a diagnosis.
Pudendal neuralgia may involve several mechanisms (multiple locks + impaired gliding + hypertonicity + sensitization). Postural improvement can be a strong indicator of a functional mechanism, without excluding structural vulnerability.
6. Conclusion
Pudendal neuralgia cannot be understood through a single explanatory lens. It results from interactions between pelvic geometry, sitting-related mechanical constraints, tissue dynamics (fascia and gliding), neuromuscular regulation (protective hypertonicity), and, sometimes, central sensitization that develops over time.
This knowledge base aims to provide robust interpretive keys: identify vulnerability zones, distinguish structural from functional mechanisms, understand referred pain, and restore coherence — a necessary condition to avoid diagnostic wandering and reconcile lived experience with explainable mechanisms.