

Introduction
Are you struggling with chronic pelvic pain, burning sensations, or a feeling of a “foreign object” in the rectum or perineum? You may have come across the term Pudendal Neuralgia—a complex and often misunderstood condition. In this article, we explore why this specific nerve is so vulnerable, how postural imbalances or chronic stress can trigger your symptoms, and most importantly, the actionable steps you can take to reclaim your daily comfort.
How to Read This Article
- ✔ Purpose: Explain the biomechanical and neuro-fascial mechanisms of pudendal neuralgia.
- ✔ Goal: Help you understand why pain is often posture- and position-dependent.
- ✔ Use: Support informed discussion with your healthcare provider.
- ✖ Limitation: This article does not replace medical diagnosis or clinical care.
1. The Pudendal Nerve: An Ultra-Sensitive “Electrical Cable”
The pudendal nerve is much more than a simple signal conductor. It is the central pivot for regulating your pelvis, managing both voluntary functions (such as pelvic floor coordination) and involuntary ones (like bladder and bowel control). Originating from the S2, S3, and S4 sacral roots, it is involved in vital functions: urinary storage and evacuation, genital sensitivity, and pelvic floor stability.
The pudendal nerve acts simultaneously as a motor, sensory, and visceral regulator—which explains why the pain it generates is so confusing and multi-faceted.
Why is it so fragile? Because it follows a winding path through your pelvis, weaving between muscles, ligaments, and fascia. Every “turn” in this path is a potential vulnerability zone where the nerve can be compressed, stretched, or irritated.
2. Mechanical “Locks”: Where and Why Does it Get Stuck?
A. The Piriformis Muscle: A “Cushion” That Becomes a Vice
The pudendal nerve exits the pelvis by passing beneath the piriformis muscle. Normally, this muscle acts as a protective cushion. However, in cases of hypertonicity (excessive tension)—often caused by stress, prolonged sitting, or intense athletic activities (running, cycling)—it transforms into a vice.
The Consequence: The nerve is pre-compressed at its very exit, making it significantly more vulnerable throughout the rest of its journey.
Real-world example: Runners and triathletes are particularly at risk, as the piriformis can thicken and lose its elasticity over time.

An obstacle course: As shown in the diagram, the nerve does not travel in a straight line. It must weave under a muscle (1), pass through a “scissor-like” ligament structure (2), enter a narrow tunnel (3), and finally divide toward the front (4). This complex anatomy explains why a simple muscle tension can become a painful mechanical lock.
B. The Ligamentous Clamp: The “Scissors” Strangling the Nerve
After bypassing the piriformis, the nerve passes between two ligaments: the sacrospinous (front) and the sacrotuberous (back). Imagine a cable caught between the blades of a pair of scissors.
When sitting, especially with a rounded back (posterior pelvic tilt), these ligaments tighten and reduce the space available for the nerve.
The Result: The nerve is crushed, causing sharp pain, burning, or tingling sensations.
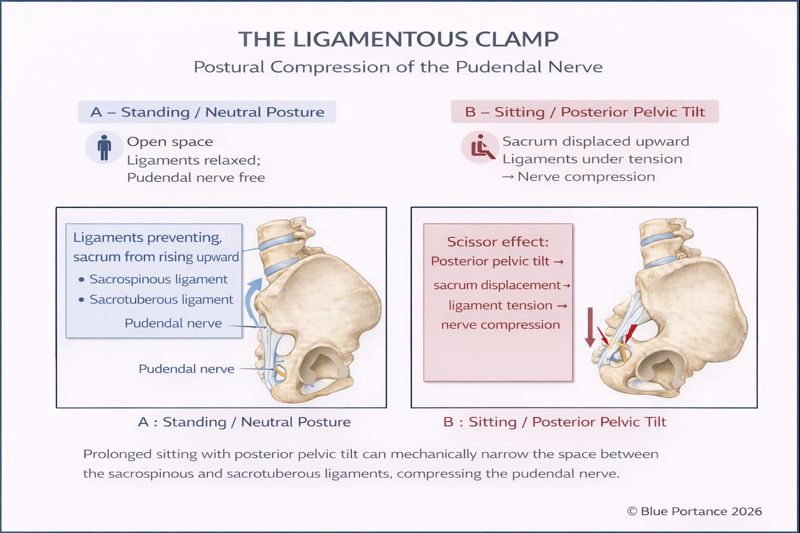
This visual highlights why posture is so delicate: the nerve is literally caught in a pincer. We often think simply “sitting up straight” is enough, but every pelvis is different. Forcing an arch that doesn’t match your natural morphology can paradoxically tighten these “scissors” further. The goal is to find the equilibrium point where these ligaments stop pinching.
Key point: Relief does not come from holding a “perfect posture,” but from restoring subtle, continuous movement within a stable range. A rigid posture—no matter how “correct”—can maintain ligament tension and perpetuate nerve compression.
C. Alcock’s Canal: A Tunnel Turned Trap
The nerve then re-enters the pelvis via Alcock’s Canal (the pudendal canal), a “tunnel” formed by the fascia of the internal obturator muscle. This canal should allow the nerve to glide freely during movement.
The Problem: If the fascia becomes inflamed (due to poor posture, childbirth, or surgery), it becomes rigid and “sticky,” trapping the nerve.
The Consequence: Every hip movement pulls on the nerve, like an electrical wire stuck in a sheath that is too tight.
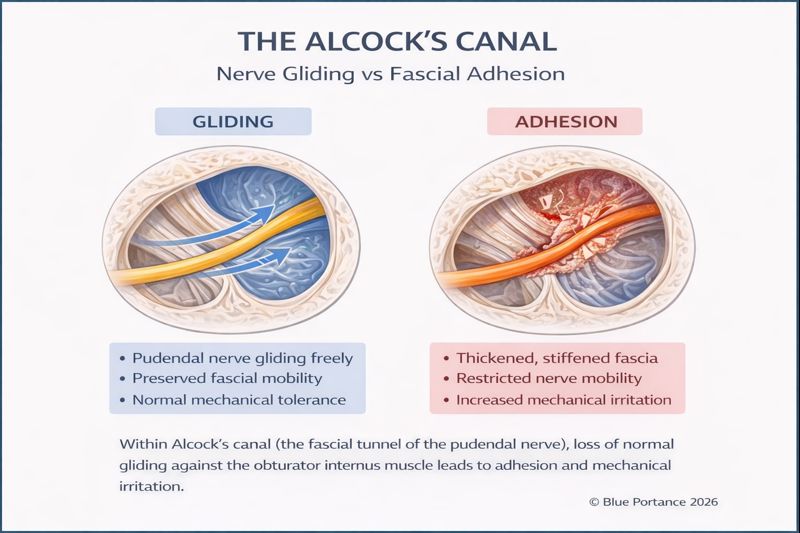
This visual brings to light a frequently ignored point: the necessity of gliding. It is estimated that 30% to 40% of tension comes not from the bone, but from the biological “glue” (fascia) surrounding the nerve. When you remain immobile for too long, these tissues densify and “clog” the nerve. This is where movement becomes therapeutic: a nerve that regains its ability to slide is a nerve that eventually stops burning.
D. The Falciform Process: An Internal “Razor Blade”
Some individuals have a fibrous extension of the sacrotuberous ligament called the falciform process. If this structure is rigid or calcified, it acts like a sharp edge irritating the nerve with every move.
Extreme Cases: In specific instances, interventions like cryoneurolysis (targeted nerve freezing) may be discussed in specialized centers to provide pain relief.
3. The Pudendal Trident: Why Pain “Travels”
Why does a pudendal neuralgia diagnosis take so long? The answer lies in the nerve’s final shape. Before reaching its destination, the pudendal nerve splits into three distinct branches, like the prongs of a trident.

One Nerve, Three Pain Zones (And Many False Leads)
Depending on which branch is most irritated, symptoms mimic common pathologies, leading medical investigations toward the organ rather than the nerve:
- The Rectal Branch (Inferior): This reaches the anal canal. It causes “razor blade” sensations, tingling, or a feeling of a foreign body in the rectum. The Trap: Patients are often treated for hemorrhoids (sometimes via surgery) even when the veins are healthy and the nerve is simply sending a false pain signal.
- The Perineal Branch (Middle): Responsible for urinary burning. Patients often undergo multiple negative urine tests (UTI/ECBU): no infection is found, only an irritated nerve. In women, this is frequently confused with endometriosis pain, delaying mechanical pelvic treatment.
- The Dorsal Branch (Superior): Innervates the genitals, causing hypersensitivity often misdiagnosed as dermatological or local infectious issues.
The Mechanism of “Referred Pain”
The trap is this: you feel the pain “at the end of the line,” but the faulty switch is located much higher in your pelvis.
This is called neuropathic pain. Like a mirage, the brain localizes pain in the rectum, bladder, or vagina, even though these organs are perfectly healthy. As long as we search for the cause only where it hurts, we remain at an impasse. To heal, we must trace back the nerve’s path and release the upstream compression zones.
4. The Role of Fascia: The Invisible Web of Tension
Fascia is the web of connective tissue linking muscles, ligaments, and nerves. They are not passive tissues; they are innervated, vascularized, and highly sensitive to mechanical load. They act as shock absorbers, but when they stiffen (due to stress, poor posture, or trauma), they transmit tension directly to the pudendal nerve.
Example: Stiffness in the hip or even the ankle can, through the fascial chains, pull on the pudendal nerve and trigger perineal pain.
Scientific Evidence: A study by Huijing (2009) showed that 30-40% of muscle forces are transmitted via fascia. This explains why pelvic pain can be linked to a blockage elsewhere in the body!
5. Stress: The Invisible Pilot
Chronic stress doesn’t just act on your mind; it alters the entire neuro-muscular-postural system.
Under prolonged stress, the autonomic nervous system stays on “high alert.” Background muscle tone increases, breathing becomes shallow, and the pelvic floor tends to contract reflexively. This persistent hypertonicity reduces movement variability and the pelvis’s ability to adapt.
In this context, fascia—already strained by posture or old injuries—loses its ability to glide. Stress acts as a systemic amplifier: it doesn’t create the lesion, but it facilitates the installation and chronicity of existing mechanical imbalances.
6. Adaptive Capacity: Why Does the Cup Overflow?
Your pudendal nerve has a limited capacity to absorb “aggressions” (poor posture, stress, scars). When the sum of these factors exceeds your adaptive reserve, pain appears.
Visualize a jar being filled with stones:
- “Structural” Stones: Unfavorable anatomy (narrow ligamentous clamp from birth).
- “Functional” Stones: Posture, stress, muscle tension.
The Goal: While you cannot change your anatomy, you can remove the “functional stones” to prevent the jar from overflowing.
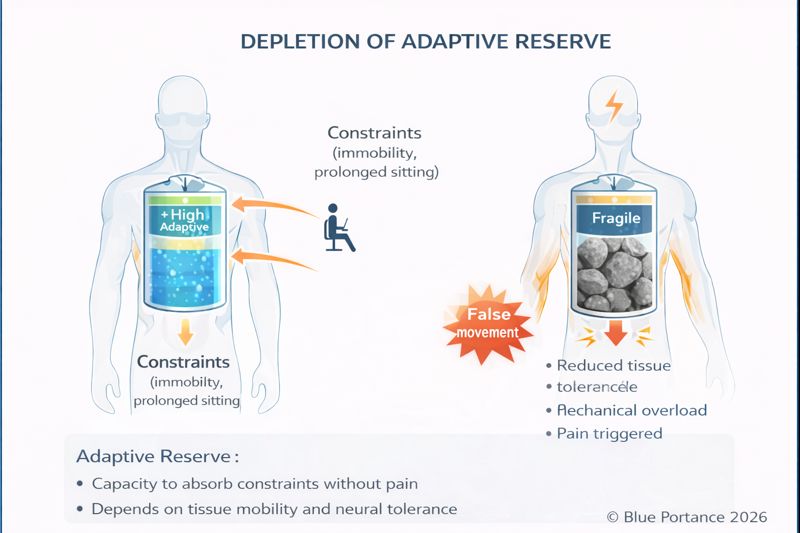
The goal of our approach is not just to “hide the symptom,” but to restore your adaptive reserve. By freeing the nerve and returning movement to the pelvis, we give your body the “breathing room” it needs to function without suffering.
Structural vs. Functional: Knowing the Difference
To effectively address pudendal neuralgia, it is essential to distinguish between structural and functional causes. This determines your recovery strategy.
🔒 Structural — “The Iron Cage”
The nerve is trapped by a fixed physical barrier: calcifications, surgical scarring, or anatomical anomalies (falciform process). These cannot be resolved by conservative approaches alone.
How to recognize it?
- Pain is present immediately upon waking, regardless of position.
- History of trauma or pelvic surgery.
- Imaging or diagnostic nerve blocks suggest a physical obstruction.
Therapeutic Direction
Requires specialized intervention and expert medical evaluation.
🟢 Functional — “The Rubber Cage”
The nerve is anatomically healthy but constrained by its environment: tight muscles, rigid fascia, or poor biomechanics.
How to recognize it?
- Pain is position-dependent (worse when sitting).
- No pain at night (A key “Nantes Criterion”).
- Pain improves with movement or postural adjustments.
👉 Functional management is the focus of the next chapter, dedicated to movement restoration and pelvic adaptability.
7. What Can I Do to Relieve the Pain?
p> Understanding the mechanisms of compression—whether it involves a ligamentous clamp, a fascial canal that has lost its ability to glide, or adhesions that have developed over time—fundamentally changes the way pudendal pain should be addressed. Relief does not come from searching for a single, rigid “correct posture,” but from identifying which constraints are functionally reversible and which require specific medical attention. Whenever possible, the goal is to restore space, movement, and adaptability around the nerve, allowing it to regain its capacity to glide and tolerate load. This principle—often referred to as micro-movement—plays a central role in relieving mechanically driven nerve pain. You can explore this concept in more detail in our dedicated article: Why Micro-Movement Matters More Than Perfect Posture .A. Correct Your Posture
- Avoid prolonged sitting with a “slumped” or rounded back.
- Use an ergonomic cushion or a dynamic seat (like those from Aporia) to maintain a neutral pelvis.
- Move regularly: Stand up every 30 minutes to walk or stretch.
B. Relax Muscles and Fascia
- Self-Massage: Use a tennis ball to gently massage the piriformis or internal obturator muscle.
- Stretches: Practice the “Figure-4” piriformis stretch.
- Diaphragmatic Breathing: To lower stress and naturally drop the pelvic floor.
C. Specialized Dynamic Seating
For functional cases, dynamic seating is a game-changer. Unlike static chairs, they:
- Stimulate Micro-movements: Preventing fascia from stiffening.
- Find the “Zero Point”: Allowing the pelvis to balance where mechanical stress is lowest.
- Reduce Compression: Targeted decompression zones limit pressure on critical nerve points.
8. Summary: Understand to Act
- Your pudendal nerve is sensitive due to its complex path.
- Posture, stress, and tension are the primary “aggravators.”
- You can influence functional factors to reduce pain, regardless of your anatomy.
A Message of Hope: Pudendal neuralgia is not a life sentence. By addressing the modifiable causes, you can reclaim your comfort and quality of life.